Abstract
Total knee arthroplasty (TKA) is an effective surgical treatment for advanced osteoarthritis, but postoperative recovery is frequently limited by quadriceps weakness, muscle atrophy, and prolonged rehabilitation. Anabolic steroids, such as nandrolone decanoate and testosterone, have demonstrated potential benefits in enhancing muscle strength, functional mobility, and bone density. This systematic review, conducted according to PRISMA guidelines and registered with PROSPERO, evaluated the efficacy and safety of anabolic steroid interventions in patients undergoing TKA. Two randomized controlled trials were identified: one assessed postoperative nandrolone administration, and the other evaluated preoperative supraphysiological testosterone therapy. Both studies reported improvements in quadriceps strength, functional outcomes, and early recovery parameters, with favorable safety profiles and no major adverse events. Nandrolone was associated with higher Knee Society Scores and reduced muscle weakness over 12 months, while testosterone improved early functional independence and shortened rehabilitation needs. Although encouraging, the findings are limited by small sample sizes, variability in dosing regimens, and short follow-up durations. Larger, multi-center studies are warranted to confirm efficacy, optimize treatment protocols, and assess long-term safety. Anabolic steroids may represent a promising adjunct to rehabilitation strategies in selected TKA patients, particularly older adults at risk of poor recovery.
Keywords: Total knee arthroplasty, anabolic steroids, quadriceps strength, functional recovery, testosterone, nandrolone
Introduction
Total knee arthroplasty (TKA) is a highly effective procedure for treating severe osteoarthritis and improving patients’ quality of life by alleviating pain and restoring mobility. However, patients, particularly older adults, often face significant challenges during recovery, including muscle atrophy, reduced functional mobility, and prolonged rehabilitation times. Preoperative disuse atrophy and postoperative muscle weakness, especially in the quadriceps, have been linked to slower recovery and diminished outcomes. After TKR, quadriceps weakness is most commonly seen especially in elderly patients, even following extensive rehabilitation1,2. This leads to functional limitation despite successfully done TKR. Exploring therapeutic strategies to enhance recovery and functional performance after TKA is essential.
Androgenic anabolic steroids are a class of compounds chemically related to testosterone, the male sex hormone. They are characterized by their effects of promoting muscle growth (anabolic properties)3 and inducing masculinization (androgenic properties). Anabolic steroids, such as nandrolone decanoate and testosterone, have well-documented anabolic effects on muscle mass and strength. Evidence from studies on athlete populations indicates that anabolic androgen use can lead to significant increases in lean body mass and strength, with gains reaching up to 20%4. Historically associated with athletic performance enhancement, their potential in clinical rehabilitation contexts, including TKA recovery, has gained interest4. This review evaluates the impact of anabolic steroid interventions on muscle recovery, functional outcomes, bone density, and hospital stay duration following TKA.
Methods
The study was registered on the PROSPERO International Prospective Register of systematic reviews. Preferred Reporting Items for Systematic Reviews and Meta-Analyses criteria were used to perform the study5. From conception of database until November 2024, two reviewers (VP and DK) searched the four Internet databases (PubMed, Embase, Scopus, and The Cochrane Library). No restrictions were applied based on language or publication status. The key terms used for searching the databases were: “anabolic steroids,” “androgenic anabolic steroids,” “Total knee arthroplasty,” “TKA,” “Total knee replacement,” “TKR.” We also manually scanned the bibliographies of the included articles for other relevant studies. For further relevant research, references from published original articles and earlier studies were searched (Table 1) and depicted in the PRISMA chart in figure-1.
Table 1: Search Methodology
| DATABASE |
DATE: 25/11/2024 |
TOTAL RESULTS = 23 |
| PUBMED |
(“anabolic androgenic steroids”[MeSH Terms] OR (“anabolic”[All Fields] AND “androgenic”[All Fields] AND “steroids”[All Fields]) OR “anabolic androgenic steroids”[All Fields] OR (“anabolic”[All Fields] AND “steroids”[All Fields]) OR “anabolic steroids”[All Fields]) AND (“arthroplasty, replacement, knee”[MeSH Terms] OR (“arthroplasty”[All Fields] AND “replacement”[All Fields] AND “knee”[All Fields]) OR “knee replacement arthroplasty”[All Fields] OR (“total”[All Fields] AND “knee”[All Fields] AND “replacement”[All Fields]) OR “total knee replacement”[All Fields]) |
4 |
| SCOPUS |
( TITLE-ABS-KEY ( anabolic AND steroids ) OR TITLE-ABS-KEY ( androgenic AND anabolic AND steroids ) AND TITLE-ABS-KEY ( total AND knee AND replacement ) OR TITLE-ABS-KEY ( tkr ) ) |
5 |
| EMBASE |
(anabolic AND steroids OR androgenic) AND steroids AND total AND knee AND replacement |
6 |
| COCHRANE |
(anabolic steroids):ti,ab,kw OR (androgenic anabolic steroids):ti,ab,kw AND (total knee arthroplasty):ti,ab,kw AND (TKR):ti,ab,kw |
8 |
Study Characteristics
- Hohmann et al6 conducted a prospective double-blind pilot study investigating the effects of 50 mg nandrolone decanoate administered bi-weekly for six months postoperatively. The study included 10 patients (5 in the treatment group and 5 controls) aged between 50 and 70 years.
- Amory et al7 performed a double-blinded, placebo-controlled trial assessing the impact of preoperative supraphysiological testosterone administration (600 mg testosterone enanthate weekly for 4 weeks) in 25 men aged 55 and older undergoing TKA.
- Functional and strength assessments were performed preoperatively and at multiple postoperative intervals, ensuring robust monitoring of recovery trajectories.
Table 2: Details of the studies included
| Study |
Study design |
No. of participants |
Intervention |
Outcome |
| Hohmann et al |
Prospective Randomised double blind trial |
10 |
50mg nandrolone decanoate I.M twice weekly for 6 months |
Knee society score8, Functional test- sit to stand, timed walk, Bone mineral density, Isokinetic strength testing |
| Amory et al |
Prospective Randomised placebo controlled double blind trial |
25 |
600mg testosterone enanthate intra muscularly once weekly for 4 weeks preoperatively |
Length of hospitalization, Functional recovery- standing, walking and stair climbing |
Results
Muscle Strength and Functional Outcomes
-
Hohmann et al.
- Patients in the nandrolone group showed significantly greater quadriceps strength at 3 months (p = 0.02), 6 months (p = 0.01), and 12 months (p = 0.02) compared to controls.
- Functional tests, including the sit-to-stand and timed walking tests, showed trends toward improved performance in the nandrolone group. However, these differences were not consistently statistically significant.
- The Knee Society Score (KSS) was significantly higher in the nandrolone group at 6 weeks (p = 0.02), 6 months (p = 0.02), and 12 months (p = 0.01), indicating better functional recovery.
-
Amory et al.
- Preoperative testosterone administration significantly improved early postoperative FIM scores for standing ability (5.2 ± 1.0 vs. 4.1 ± 1.1, p = 0.04). Trends toward better walking and stair-climbing abilities were also noted.
- By postoperative Day 35, 31% of patients in the testosterone group achieved FIM scores equal to or better than their baseline, compared to 18% in the placebo group.
Bone Mineral Density
- Hohmann et al. observed a lower percentage decrease in bone mineral density in the nandrolone group compared to controls (femur: 0.71% vs. 3.8%; spine: 1.25% vs. 1.97%). However, these differences were not statistically significant.
Hospital Stay and Rehabilitation
- Amory et al. reported a nonsignificant reduction in hospital stay duration for the testosterone group (5.9 ± 2.4 days vs. 6.8 ± 2.5 days). Fewer patients in the testosterone group required inpatient rehabilitation compared to the placebo group (20% vs. 25%).
Safety and Side Effects
A key strength of the reviewed studies is the favourable safety profile of anabolic steroids in the studied populations. Both nandrolone and testosterone were well-tolerated, with no major adverse events reported. Minor side effects, such as hematocrit fluctuations, were observed but deemed clinically insignificant. However, it is important to recognize that long-term use of anabolic steroids, particularly at supraphysiological doses, has been associated with potential endocrine, cardiovascular, and hepatic risks9,4. Therefore, careful monitoring of patients receiving anabolic steroids is necessary to ensure safety, especially in older adults with preexisting comorbidities.
Discussion
Implications of Findings
The findings from the reviewed studies underscore the promising role of anabolic steroids, such as nandrolone and testosterone, in enhancing recovery after total knee arthroplasty (TKA). A consistent benefit observed in both studies was the improvement in muscle strength, particularly in the quadriceps, which is crucial for post-TKA functional recovery. Quadriceps weakness has been widely documented as a major contributor to prolonged rehabilitation times and reduced functional outcomes following TKA, particularly in older adults2. By counteracting muscle atrophy and promoting strength recovery, anabolic steroids address a critical challenge in postoperative care.
The study by Hohmann et al. demonstrated that patients receiving nandrolone decanoate exhibited significant improvements in quadriceps strength at multiple time intervals postoperatively (3 months, 6 months, and 12 months). This result is clinically significant because muscle strength recovery is directly linked to improved functional outcomes, such as walking ability, sit-to-stand performance, and stair-climbing. The Knee Society Score (KSS), a validated measure of knee function and pain, was also notably higher in the nandrolone group, reinforcing the potential benefits of anabolic steroids in improving overall knee performance.
Similarly, the findings of Amory et al. highlight the benefits of preoperative testosterone administration which exhibited enhanced early recovery, particularly in functional independence measures (FIM) such as standing, walking, and stair climbing. This early functional recovery can significantly reduce rehabilitation times and improve patient independence. While the improvements in walking and stair-climbing were not always statistically significant, trends in favour of anabolic steroid use were consistently observed, suggesting a meaningful clinical benefit even in small sample sizes.
An additional benefit observed in the studies was the potential role of anabolic steroids in preserving bone mineral density (BMD)10,11. Hohmann et al. reported a smaller decrease in BMD in patients receiving nandrolone compared to controls, although the difference was not statistically significant. Maintenance of bone density is an important factor in long-term recovery, as reduced BMD can increase the risk of periprosthetic fractures, particularly in older adults with osteoporosis12. Further studies are needed to determine the magnitude and consistency of this benefit.
Mechanisms of Action
The beneficial effects of anabolic steroids can be attributed to their physiological mechanisms. These compounds exert their anabolic effects by enhancing protein synthesis, leading to increased muscle mass and strength. In the postoperative period, anabolic steroids may accelerate muscle recovery by promoting muscle protein anabolism13, counteracting catabolic processes associated with surgical stress and immobilization.
Furthermore, testosterone, in particular, has additional systemic benefits, such as improving hematopoiesis14 and increasing red blood cell mass, which may contribute to enhanced oxygen delivery and improved endurance during rehabilitation. This effect may also reduce the need for blood transfusions, which are often required after major surgeries like TKA, particularly in older adults. The ability of testosterone to address multiple physiological aspects makes it a potentially valuable adjunct to traditional rehabilitation strategies.
Limitations
Despite the encouraging results, several limitations must be acknowledged. Both studies included in this review had relatively small sample sizes, which limit the generalizability of their findings. For instance, Hohmann et al. included only 10 patients, while Amory et al. had a sample size of 25. Larger, multi-center trials are necessary to confirm these findings and establish more robust evidence.
Additionally, there was variability in the dosing regimens and timing of administration across the studies. Hohmann et al. administered nandrolone bi-weekly for 6 months postoperatively, while Amory et al. used a supraphysiological dose of testosterone preoperatively for 4 weeks. This heterogeneity makes it challenging to determine the optimal dosing regimen and treatment duration for maximizing benefits. Standardized protocols are needed to facilitate comparisons across studies and guide clinical practice.
The short duration of follow-up in both studies is another limitation. While improvements in muscle strength and functional outcomes were observed in the short term, the long-term effects of anabolic steroids on functional recovery, bone health, and overall quality of life remain unclear. Long-term follow-up is crucial for evaluating the sustainability of benefits and identifying any delayed adverse effects.
Future Directions
To better understand the role of anabolic steroids in TKA recovery, future research should:
- Include larger, multi-center trials with diverse patient populations.
- Investigate optimal dosing regimens, treatment durations, and combinations with other rehabilitation strategies.
- Assess long-term safety profiles, particularly concerning bone health and potential endocrine or cardiovascular side effects.
Conclusion
Anabolic steroids, such as nandrolone and testosterone, show promise in enhancing postoperative recovery following TKA by improving muscle strength and functional mobility. By improving muscle strength, functional outcomes, and possibly bone density, anabolic steroids hold significant promise for enhancing recovery, particularly in older adults at risk of prolonged rehabilitation. However, further large-scale, high-quality studies are needed to confirm these findings, establish clear treatment guidelines, and ensure the long-term safety of anabolic steroid use in clinical practice.
Bibliography
- Stevens JE, Mizner RL, Snyder-Mackler L. Quadriceps strength and volitional activation before and after total knee arthroplasty for osteoarthritis. J Orthop Res Off Publ Orthop Res Soc. 2003 Sep;21(5):775–9.
- Mizner RL, Petterson SC, Snyder-Mackler L. Quadriceps strength and the time course of functional recovery after total knee arthroplasty. J Orthop Sports Phys Ther. 2005 Jul;35(7):424–36.
- Sinha-Hikim I, Artaza J, Woodhouse L, Gonzalez-Cadavid N, Singh AB, Lee MI, et al. Testosterone-induced increase in muscle size in healthy young men is associated with muscle fiber hypertrophy. Am J Physiol Endocrinol Metab. 2002 Jul;283(1):E154-164.
- Hartgens F, Kuipers H. Effects of androgenic-anabolic steroids in athletes. Sports Med Auckl NZ. 2004;34(8):513–54.
- Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol. 2009 Oct;62(10):1006–12.
- Hohmann E, Tetsworth K, Hohmann S, Bryant AL. Anabolic steroids after total knee arthroplasty. A double blinded prospective pilot study. J Orthop Surg. 2010 Dec 15;5:93.
- Amory JK, Chansky HA, Chansky KL, Camuso MR, Hoey CT, Anawalt BD, et al. Preoperative supraphysiological testosterone in older men undergoing knee replacement surgery. J Am Geriatr Soc. 2002 Oct;50(10):1698–701.
- The Knee Society Score [Internet]. [cited 2024 Dec 15]. Available from: https://www.kneesociety.org/the-knee-society-score
- Bond P, Smit DL, Ronde W de. Anabolic–androgenic steroids: How do they work and what are the risks? Front Endocrinol. 2022 Dec 19;13:1059473.
- Adachi M, Takayanagi R. [Effect of anabolic steroids on osteoporosis]. Clin Calcium. 2008 Oct;18(10):1451–9.
- Orwoll ES. Androgens as anabolic agents for bone. Trends Endocrinol Metab. 1996 Apr 1;7(3):77–84.
- Fink HA, Ewing SK, Ensrud KE, Barrett-Connor E, Taylor BC, Cauley JA, et al. Association of testosterone and estradiol deficiency with osteoporosis and rapid bone loss in older men. J Clin Endocrinol Metab. 2006 Oct;91(10):3908–15.
- Bhasin S, Woodhouse L, Casaburi R, Singh AB, Bhasin D, Berman N, et al. Testosterone dose-response relationships in healthy young men. Am J Physiol Endocrinol Metab. 2001 Dec;281(6):E1172-1181.
- Singer JW, Adamson JW. Steroids and Hematopoiesis. III. The Response of Granulocytic and Erythroid Colony-forming Cells to Steroids of Different Classes. Blood. 1976 Dec 1;48(6):855–64.
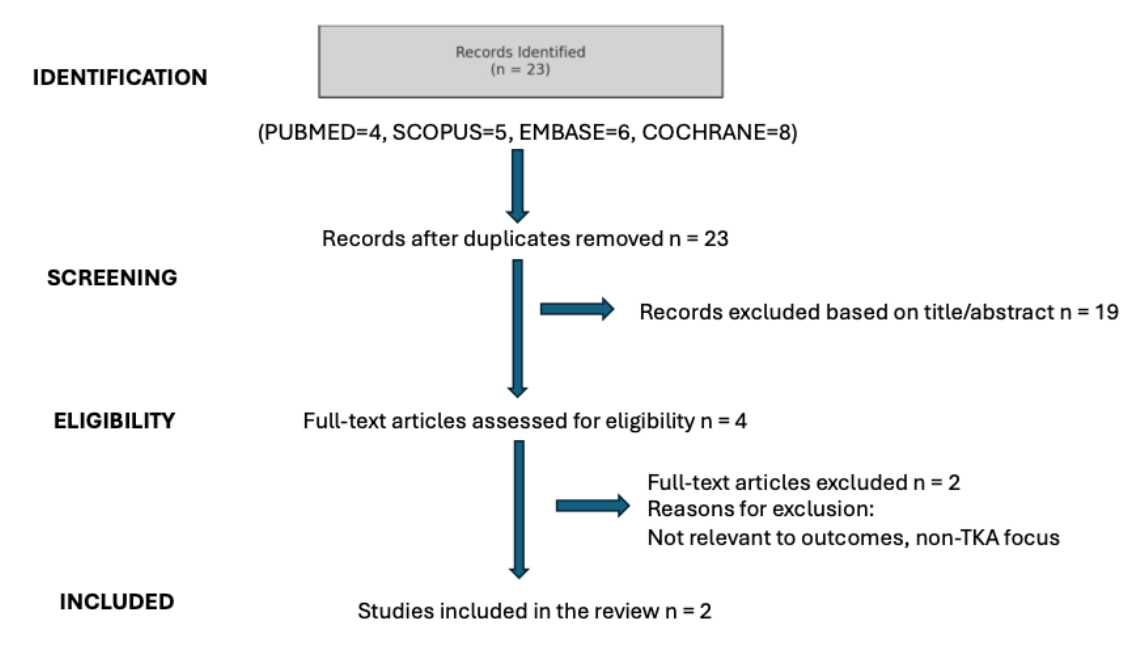
Figure 1: PRISMA chart depicting the process of literature review
