Welcome to International Journal of Geriatric Orthopedics (IJGO)
The Impact of Osteoporosis and Sarcopenia on Spine in Causing Pain and Altered Biomechanics
Dr. Prabodh kumar dake, Dr. Bhaswanth dake, Dr. Lavanya kumari sarella
Abstract
Back pain is a very common complaint made by the middle aged and geriatric age group patients in orthopaedic practice. As age advances most of the middle and old aged men and women suffer from neck pain and back pain (upper back, mid back, lower back). Purpose of study is to evaluate the role of osteoporosis and sarcopenia in causing back pain and its impact on spine biomechanics.
Key words: osteoporosis, sarcopenia
Introduction
Osteoporosis and sarcopenia are very common problems in older individuals. These two clinical conditions are interlinked. Muscles can contract with good tone when bone is strong enough and when the bones are porotic, muscles cannot contract effectively. Load bearing capacity of facet joints depends on strength of the bone and strength of the paraspinal muscles. Sarcopenia causes early muscle fatigue and failure of load bearing capacity and thus load falls directly on vertebrae. This significantly affects the quality of life and limits the individual activity. Unfortunately, there is a common misconception among many physicians that these pains are due to osteoarthritis of spine as a result of facet joint degeneration due to ageing.
Aim of the study: to prove that the cause of pain at back in older people is mainly due to osteoporosis and sarcopenia and how it impacts on biomechanics of spine.
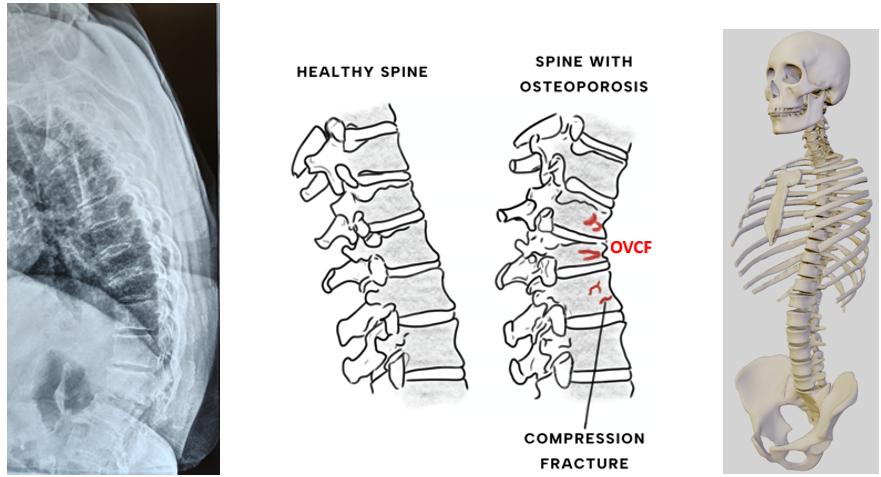
Osteoporosis: Albright said long time ago, in simple terms that osteoporosis is “Too little bone, but what bone there is, is normal”. Osteoporosis is a widespread systemic skeletal disease in geriatric population where not only the bone mass but also the bone quality is affected. Indian society for bone and mineral research (ISBMR) defines osteoporosis is a condition characterised by low bone mass and micro-architectural deterioration of bone tissue, with a consequent increase in bone fragility and susceptibility to fracture. In osteoporotic bone not only the cortical bone gets thinner but also the trabeculae become sparse, thin and break thus making the bones vulnerable to fractures. According to World Osteoporosis Foundation data [1], one in three women and one in five men over 50 may experience an osteoporosis related fracture in their life time. Statistics reveals that 4 out of 10 women after the age of 50 sustain at least one osteoporotic fracture. Most common sites involved are distal radius, the spine, proximal femur and proximal humerus [2].
In childhood and adolescent period bone formation exceeds resorption, resulting in continued skeletal growth and peak bone mass is attained at about 30 years of age. After this, resorption begins to exceed formation. Normal bone loss averages 0.7 percent per year. It gets enhanced at the time of menopause to 2-5 percent per year. Studies have suggested that genetic component is responsible for bone mass may be linked to polymorphism in the gene for vitamin D receptor [3]. Important nutritional factors include dietary calcium, protein intake, vitamin D, vitamin C, vitamin K status, and minerals like copper, zinc and manganese play an important role in formation of bone mineral mass [4].
Cortical bone makes up approximately 80% of the skeleton, while trabecular (cancellous) bone constitutes only 20% of the skeleton. The trabecular bone has a much larger surface area than cortical bone because of its honey comb like structure, example; vertebral body [5]. Bone loss occurs as a result of alterations in remodelling. Increase in function and life span of osteoclasts can lead to a greater number of remodelling sites (resorption sites) that cannot be adequately filled by osteoblasts. This high turnover bone loss is most common in postmenopausal women. Loss of estrogen with menopause leads to increased production of several cytokines responsible for the proliferation and differentiation of osteoclasts. These cytokines have also been shown to inhibit osteoclast apoptosis. Since the trabecular bone is more metabolically active, it tends to be affected by high turnover. High bone turnover is considered as an independent risk factor for fractures.
Bone is a dynamic living tissue which gives structural support, protection of internal organs, facilitation of movement, storage of minerals (mainly calcium and phosphate) and housing of bone marrow for haemopoiesis. The bone is composed of organic (matrix of bone) and inorganic (mineral) components. Collagen type -1 is most abundant protein in the organic matrix of the bone that amounts up to 90-95% of the total bone collagen content. It is important to provide structural frame work for the minerals and to support overall bone remodelling process. Hence it is very essential to have enough collagen in the body to ensure the optimal bone health. It has been observed that osteoporotic bones show decreased collagen level leading to a weaker bone matrix and increased susceptibility to fractures. P1NP (procollagen type1 amino terminal propeptide) is a reliable biomarker to know the level of collagen formation in the body. Supplements that can improve P1NP level in body can be considered to be supporting the collagen production in bone.
It is interesting to note that a number of elderly osteoporotic patients also suffer from osteomalacia as evidenced by the presence of thick osteoid. This combination of osteoporosis and osteomalacia is referred to as ‘Poromalacia’. Osteoporosis is a ‘silent epidemic’ and the incidence is increasing the world over due to increase in longevity. Every year, October 20th is celebrated as ‘World Osteoporosis Day’ to create awareness of the ‘burden of the disease on the society.
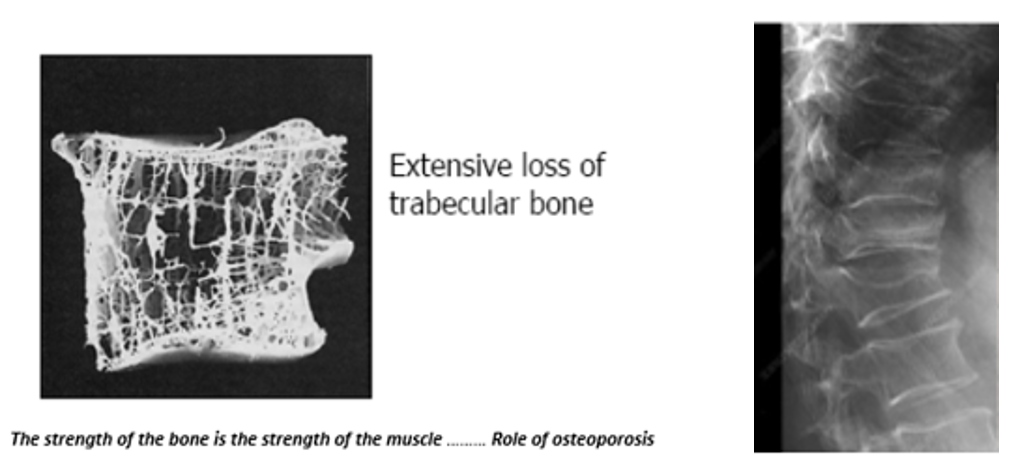
Thinned cancellous trabeculae break and collapse
Sarcopenia… Sarcopenia is a progressive and generalized loss of skeletal muscle mass and function. The prevalence of sarcopenia was reported to be up to 29% in older persons. Sarcopenia diagnosis is confirmed by the presence of low muscle mass and low muscle strength or low physical performance. Sarcopenia can greatly impact quality of life by reducing ability to perform daily activities. Spine extensor muscles extend the spinal column to enable actions like standing and bending backward. The primary extensors are erector spinae group, along with deep muscles like the multifidus and semispinalis. Other muscles contributing to extension includes the quadratus lumborum and the gluteal muscles. The chief flexors of spine are rectus abdominis and also internal oblique, external oblique and the psoas major muscles. Paraspinal muscle degeneration and increased fat infiltration lead to loss of muscle strength and endurance. The paraspinal muscles play an important role in maintaining the balance of spine. Sarcopenia can impact a person’s back, chest and abdomen by causing atrophy and degeneration of the paraspinal muscles, leading to back pain, spinal instability, and postural issues like thoracic kyphosis. Sarcopenia of chest muscles and intercoastal muscles can cause pulmonary issues like reduced vital capacity of lung and sarcopenia of spine flexor muscles can cause bowel motility problems. This muscle loss in the back, known as spinal sarcopenia, is a recognized clinical condition that can worsen with age and contribute to a reduced quality of life.
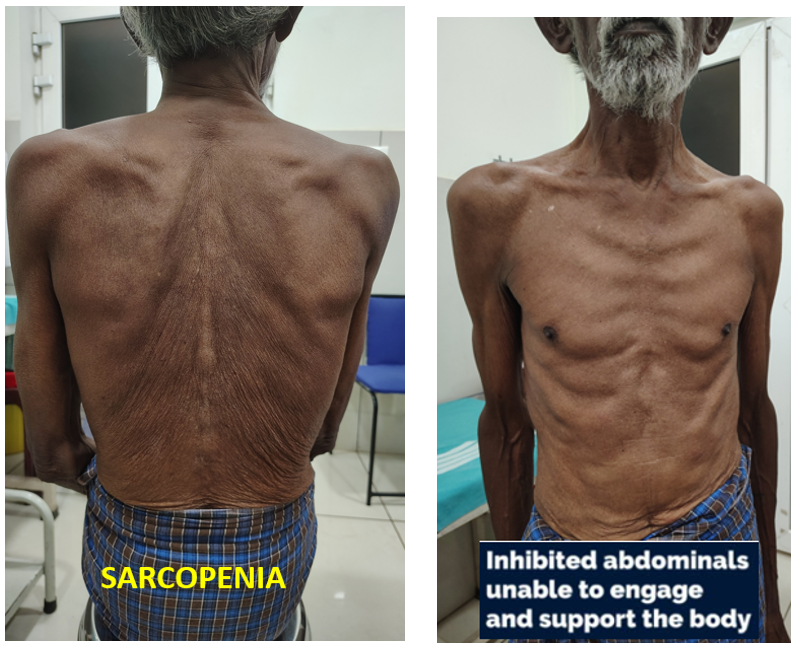
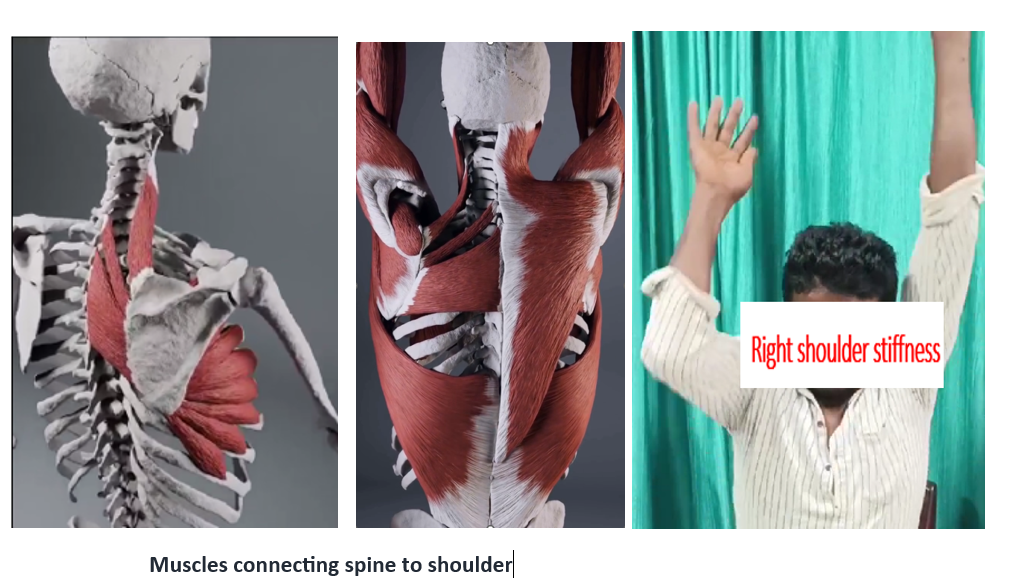
Osteoporosis and sarcopenia influence the weight bearing and load bearing capacity of joints especially facet joints of spine, vertebrae. Due to sarcopenia and osteoporosis, the load bearing capacity of para spinal muscles reduced, hence weight falls directly over the vertebrae which in turn cause the collapse of cancellous trabeculae by microfractures and the height of the vertebrae is reduced and assume kyphotic deformity at cervicothoracic junction, lower thoracic and lower lumbar spine which alters biomechanics of spine. hence the para spinal muscles become lax and unable to contract with good tone and fail in load bearing. Hence the muscle fatigue due to sarcopenia and microfractures due to osteoporosis gives pain at load bearing regions especially at lower cervical, lower thoracic and lower lumbar regions where they take maximum axial load. Pain is more in prolonged sitting and standing. Sarcopenia of the back muscles those connecting spine and shoulders which can cause inability of shoulders to maintain upright position and further causes stiffness of shoulders and juxta-articular osteoporosis. Patient suffers from limitation of shoulder joint movements and pain.
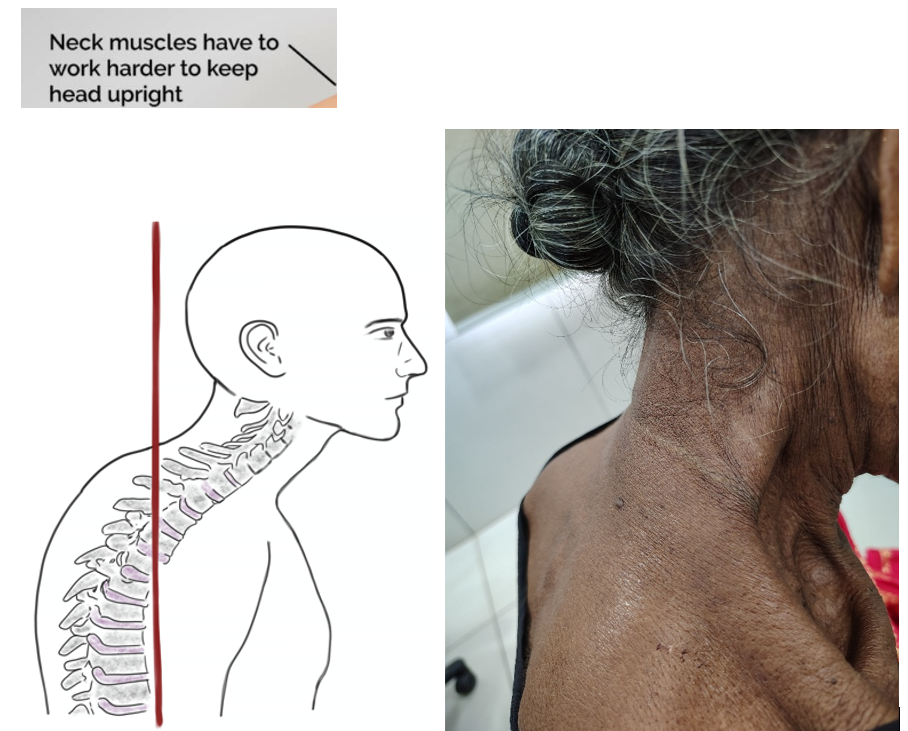
Sarcopenia and Osteoporosis cause difficulty in neck holding. For every inch of forward head posture, it can increase the weight of the head on the spine by an additional 10 pounds.
Due to sarcopenia and osteoporosis the skeleton undergoes several adaptive structural changes, such as bone mass loss which is accompanied by sarcopenia and results in early fatiguability and immobility. Muscle weakness causes more load on spine leads to axial kyphosis and continuous loss of bone mass. Fragility and sarcopenia may lead to multiple osteoporotic vertebral compression fractures (OVCFs) and continuous contraction of paravertebral muscles to maintain body posture which results in progressive kyphotic deformity. This will cause muscle fatigue and persistent pain. Fracture vertebra is the most common finding in patients with osteoporosis and sarcopenia. About 12% of the postmenopausal women encounter at least one vertebral fracture leading to deformity. Osteoporotic vertebral compression fracture (OVCF) jeopardizes the geriatric group especially postmenopausal women are more susceptible and about 40% of women experience OVCFs in their life time [6]. The OVCFs and adjacent vertebral compression fractures may result in pain, kyphosis and sometimes neurological impairment may severely affects patients’ quality of life.
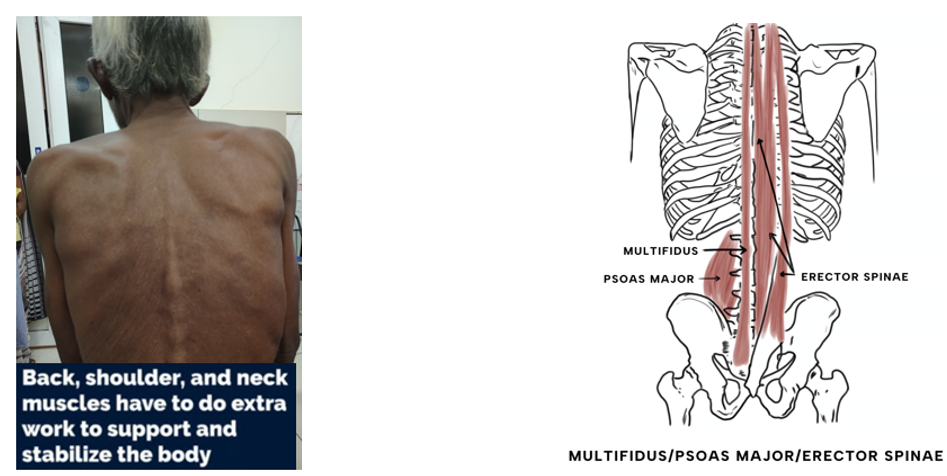
Among the paraspinal muscles, the multifidus muscle is a crucial stabilizer of spine. Hence the sarcopenia of multifidus muscle plays a major role in causing OVCFs. The paraspinal muscles are primarily composed of multifidus, erector spinae and psoas muscle. They are responsible for providing dynamic stability to the spine. They play a major role in maintaining the balance of spinal alignment. Among these paraspinal muscles multifidus muscle is the innermost and largest one and is responsible for two thirds of the spinal stability for its unique morphology. The multifidus is a deep, thin, but vital muscle that runs along the entire length of the spine, most developed in the lumbar region. It functions as a local core stabilizer, playing a key role in spinal stability, posture, and movement. Weakness in the multifidus is associated with low back pain. Its sarcomeres are positioned on the ascending portion of the length tension curve, allowing the muscle to become stronger as the spine assumes a forward learning posture.
Multifidus has closer anatomical connections to the vertebral laminae and spinous process. Thus, its ability to control lumbar spine movements may be a crucial factor to cause back pain. Based on its above characteristics, multifidus is a crucial stabilizer of spine and its degeneration can cause multiple OVCFs. Multifidus muscle is one of the key stabilizing muscles of spine and the disruption of its motor control system can cause the functional instability of spine which in turn leads to overloading of the vertebral joints which ultimately cause OVCF and severe pain. OVCF is often accompanied by severe paraspinal muscle atrophy. Sarcopenia and intramuscular fat are associated with poor muscle strength which weakens the ability of paraspinal muscles to maintain spinal alignment [7].
Impact of osteoporosis and sarcopenia on spine biomechanics
The skull, spine, and pelvis form the central axis of the human skeleton. The spine is balancing the cranium above with the help of neck muscles and it is maintaining the vertical axis with the support of pelvis at the base of the spine. The spine is holding neural tissue (spinal cord and cauda equina). The trunk (chest) and pelvis also attached to spine which holds important organs like heart, lungs, gastrointestinal system and pelvic organs respectively. Osteoporosis and sarcopenia alters biomechanics of spine which indirectly affects movements of chest wall and abdomen. This may cause reduction in pulmonary function and bowel movement.
Sarcopenia causes weakness and early fatigue of back muscles which holds spine erect and shoulders in upright position. Hence this failure of load bearing capacity of the back muscles leading to load falling directly on osteoporotic vertebrae which in turn produce compression fractures results in kyphosis. Shoulders assume drooped position and become stiff. Upright posture becomes difficult. This bending posture alters gait and flexion contractures develop at hip and knee as patient walks in bending posture to balance himself.
Clinically, the onset of symptoms due to osteoporosis is very insidious – generalized body aches especially upper back, mid back, low back ache and a slow increase in dorsal kyphosis. Patients with osteoporosis and sarcopenia, present with chronic musculoskeletal pain especially at back along with axis of spine, gluteal region and at scapulohumeral regions which lead to disability and impairment in quality of life. The most common complaints made by geriatric population suffering from osteoporosis and sarcopenia are back pain, spine deformity, postural imbalance and muscle fatigue.
The peripheral nervous system supplies the skeletal system abundantly and is responsible for pain generation and modifying bone homeostasis, predominantly in osteoporosis [8]. In older age group the balance between osteoblastic and osteoclastic activity become reverse and osteoclastic activity predominates. During increased osteoclastic activity, the vacuolar H+ -ATPase secretes protons, producing an acidic micro environment that breaks down bone minerals. This micro acidic environment is responsible for activation of nociceptors in bone and induce pain.
Progressive person’s height loss greater than 4cm could suggest vertebral fractures. Persistent back pain may also indicate underlying vertebral fractures. Upright posture becomes impossible. pulmonary volume loss present due to anterior wedging of spine. 12th rib rests on iliac crests or narrowed gap between ribs and ilium (less than two fingers), protruding abdomen are other common features.
Clinically vertebral fractures are associated with height loss, thoracic kyphosis, back pain, pulmonary and abdominal problems. Early diagnosis of osteoporosis is mandatory for two reasons – Firstly, if osteoporosis is diagnosed at a particular point of time at best it is possible to maintain the bone mass at that level only. Secondly, the thinned out discontinuous trabeculae may become thick with treatment but their continuity is difficult to reestablish. It is better to start treatment before their continuity is disrupted.
The muscles connecting spine to shoulder plays a major role in scapulothoracic movements and sarcopenia causes weakness of these muscles which leads to limitation of movements and stiffness of shoulder and juxta-articular osteoporosis. It produces severe pain on moving shoulder.
Management of Osteoporosis and Sarcopenia to Protect Spine
Early diagnosis and treatment of osteoporosis and sarcopenia can prevent musculoskeletal pain, OVCFs, kyphosis and quality of life can be improved.
Non Pharmacological Therapy
Physiotherapy plays a major role in reducing chronic pain in osteoporosis and sarcopenia. Different physiotherapy modalities like mechanical stimuli in the form of massage, thermal stimulation in the form of high or short-wave thermic waves and electrical stimulation in the form of direct current or low frequency electrical stimulation are very useful [9]. Yoga plays an important role in pain relief and enhancing physical and social wellbeing. Pilates exercises are useful in reversing osteoporosis and sarcopenia. Physical exercises improve muscle strength, balance, coordination and cognitive functions (10). Diathermic ultrasound improves tissue metabolism, induces hyperemia, increases tissue circulation and increases the elasticity of soft tissue fibers, finally gives pain relief. Vibration effects have also improved osteoporosis pain, neuromuscular coordination, and physical fitness [11].
Exercise therapy strengthens not only generalised muscles but also localised back muscles as potentially helpful for improving quality of life. Early management of paraspinal muscle therapy can potentially prevent OVCF. Lee et al found that improving the strength of paraspinal muscles could lead to reduction in pain and improved spinal function.
Pharmacological Therapy
As the osteoporosis is observed mainly in older people with various comorbidities, the choice of analgesics should be determined based on pain intensity and also type of pain [12]. All anti – osteoporosis medicines influence bone metabolism and help restore the normal bone structure, finally gives relief from pain.
Vitamin D
Vitamin D plays a major role in improving muscular function, osteoblastic activity, promoting dietary calcium absorption from the intestinal tract and controls calcium metabolism and parathyroid hormone action. The incidence of fractures and pain decreases as skeletal function is improved [13].
Bisphosphonates
Bisphosphonates inhibit bone resorption. Anti resorptive therapy can strengthen thinned trabeculae by filling the remodelling space, but continuity cannot be made among perforated trabeculae. They reduce pain by inhibiting the production of neuropeptides, calcitonin gene – related peptides and inflammatory cytokines (TNF- alpha) [14]. Bisphosphonates decrease bone pain, stiffness, enhances motor function and improve quality of life in postmenopausal women.
Teriparatide
Albright et al. [15] first reported that PTH stimulates bone formation in 1929. It took another 47 years to produce the hormone in pure and large quantities to conduct treatment studies. In 1976, the first clinical trial was conducted by Reeve et al [16] who treated four women with osteoporosis for 6 months and observed enhanced bone turnover.
Teriparatide is a recombinant PTH/ r PTH, contains 1-34 amino acids of the human parathyroid hormone that lowers back pain in severe osteoporosis patients and lowers the risk of vertebral fractures, disability and improves quality of life. Teriparatide accelerates fracture healing, stabilizes the fracture vertebrae and relieves pain. Teriparatide also increases bone mineral density, improves quality of life and decreases the need for analgesics [17]. Recent data suggest that teriparatide is best given as monotherapy and not in combination with a bisphosphonates. Anti resorptive medication should be prescribed following teriparatide treatment to preserve bone mass gained during treatment with teriparatide.
Surgery
Surgery is indicated to stabilise the spine, to prevent progression of kyphosis and to correct the deformity which ultimately gives pain relief. It is better to initiate pharmacological therapy before going for surgery, not only to give relief from pain but also to strengthen the spine for better fixation. Studies show that osteoporosis is a potential risk factor for post operative complications such as reoperation.
Efficacy Evaluation After Treatment
Pain/ weakness/ walking/ go stairs up and down/ raise from a chair ….. to be observed
Discussion
Osteoporosis and sarcopenia are very common musculoskeletal problems in geriatric people but more common in postmenopausal and post hysterectomised women. Muscle and bone are interdependent. Sarcopenia leads to muscle fatigue and make the person less mobile which in turn leads to osteoporosis. Strong bone is the strength of the muscle. Powerful contraction of the muscle depends on strength of the bone.
Conclusion
Neck pain, shoulder pain, mid back and low back pain and gluteal pain are mainly due to early fatigue of sarcopenic back muscles which are unable to take axial loads and also due to osteoporosis which causes micro fractures of thinned out trabeculae of vertebrae. This further causes progression of thoracic kyphosis and altered biomechanics of spine which affects the quality of life. Early diagnosis and early treatment can reverse both osteoporosis and sarcopenia and can definitely provide good quality of life.
References
- 1. Sozen, T., Ozisik, L., & Basaran, N.C. (2017). An overview and management of osteoporosis. European Journal of Rheumatology, 4(1), 46-56.
- 2. KANIS JA, MELTON LJ (III), CHRISTIANSEN C. The diagnosis of osteoporosis. J. Bone Miner. Res. (1994) 9:1137-1141.
- 3. Francis RM, Harrington F, Turner E, Papiha SS, Datta HK. Vitamin D receptor gene polymorphism in men and its effect on bone density and calcium absorption. Clin Endocrinol, 1997;46:83-6.
- 4. Nutritional factors. Adapted from URL: http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement/endocrinology/osteoprosisdisease/ Accessed on 23 Dec 2010.
- 5. Woolf AD, Dixon AS. Osteoporosis: a clinical guide. 2nd ed. London: Livery House; 1998.
- 6. Silverman SL. The clinical consequences of vertebral compression fracture. Bone 1992;13:S27-31. https://doi.org/10.1016/8756-3282(92)90193-Z.
- 7. Huang W, Cai XH, Li YR, Xu F, JIANG XH, Wang D, et al. The association between paraspinal muscle degeneration and osteoporotic vertebral compression fracture severity in postmenopausal women. Journal of Back and Musculoskeletal Rehabilitation 2023;36(2):323-9. https://doi.org/10.3233/BMR-220059.
- 8. Lerner, U. H., & Persson, E. (2008). Osteoporotic effects by the neuropeptides calcitonin gene-related peptide, substance P and vasoactive intestinal peptide. Journal of Musculoskeletal and Neuronal Interactions, 8(2), 154-165.
- 9. Lange, U., Teichmann, J., & Uhlemann, C. (2025). Current knowledge about physiotherapeutic strategies in osteoporosis prevention and treatment. Rheumatology International, 26(2), 99-106.
- 10. Angin, E., Erden, Z., & Can, F. (2015). The effects of clinical pilates exercises on bone mineral density (BMD), physical performance and quality of life of women with postmenopausal osteoporosis. Journal of Back and Musculoskeletal Rehabilitation, 28(4), 849-858.
- 11. Iwamoto, J., Takeda, T., Sato, Y., & Uzawa, M. (2005). Effect of whole-body vibration exercise on lumbar bone mineral density, bone turnover, and chronic back pain in post-menopausal osteoporotic women treated with alendronate. Aging Clinical and Experimental Research, 17(2), 157-163.
- 12. Yang, J., Bauer, B. A., Wahner-Roedler, D. L., Chon, T. Y., & Xiao, L. (2020). The modified WHO analgesic ladder: Is it appropriate for chronic non cancer pain? Journal of Pain Research, 13, 411-417.
- 13. Hou, Y. C., Wu, C.C., Lu, K. C. (2018). Role of nutritional vitamin D in osteoporosis treatment. Clinica Chimica Acta, 484, 179-191.
- 14. Iwamoto, J., Makita, K., Sato, Y., Takeda, T., & Matsumoto, H. (2011). Alendronate is more effective than elcatonin in improving pain and quality of life in postmenopausal women with osteoporosis. Osteoporosis International, 22(10), 2735-2742.
- 15. BAUER W, AUB AC, ALBRIGHT F. Studies of calcium and phosphorous metabolism. V. A study of the bone trabeculae as a readily available reserve of calcium. J. Exp. Med. (1929) 49:145-161.
- 16. REEVE J, MEUNIER PJ, PARSONS JA, et al. Anabolic effect of human parathyroid hormone fragment on trabecular bone in involutional osteoporosis; a multicentre trial. Br. Med. J. (1980) 280:1340-1344.
- 17. Manuele, S., Sorbello, L., Puglisi, N., Grasso, S., La Malfa, L., D’ Urbino, G., et al. (2007). The teriparatide in the treatment of severe senile osteoporosis. Archives of Gerontology and Geriatrics, 44(suppl l), 249-258.
