Welcome to International Journal of Geriatric Orthopedics (IJGO)
Pathological Insights into Osteoporotic Bone: Implications for Orthopaedic Practice
Dr Bushu Harna, Dr Ankush Nayyar
Authors:
- Dr Bushu Harna, Consultant Orthopaedic Surgeon, Indus International Hospital, Mohali, Punjab, India, bushu.edu@gmail.com
- Dr Ankush Nayyar, Consultant Pathologist, Indus International Hospital, Mohali, Punjab, India
Corresponding Author:
Dr Bushu Harna, Consultant Orthopaedic Surgeon, Indus International Hospital, Mohali, Punjab, India
Abstract
Osteoporosis is a major global health concern characterised by reduced bone mass and microarchitectural deterioration, resulting in increased fracture risk. Although bone mineral density (BMD) assessment remains central to diagnosis, it does not fully account for fracture susceptibility observed in clinical practice. From a pathological standpoint, osteoporosis encompasses both quantitative and qualitative alterations in bone tissue that are often underrecognized in routine orthopaedic decision-making.
Histologically, osteoporotic bone is characterised by thinning and perforation of trabeculae, reduced trabecular connectivity, increased cortical porosity, and disruption of osteocyte lacunar networks. These microscopic changes substantially compromise mechanical strength, even in individuals with borderline or modestly reduced BMD. Importantly, such alterations influence fracture healing, implant anchorage, and long-term surgical outcomes.
The burden of osteoporosis is rising rapidly, particularly among postmenopausal women and the ageing population. In India, underdiagnosis and delayed intervention remain significant challenges due to limited screening, poor awareness, and sociocultural barriers affecting women’s health. Fragility fractures frequently represent the first clinical manifestation of the disease, placing orthopaedic surgeons at the forefront of diagnosis and secondary prevention.
This article highlights the pathological basis of osteoporotic bone fragility and underscores its relevance to orthopaedic practice. A clear understanding of the microscopic substrate of osteoporosis can help surgeons anticipate surgical challenges, optimise fixation strategies, and foster interdisciplinary collaboration for comprehensive patient care.
Introduction
Osteoporosis is a systemic skeletal disorder characterised by decreased bone mass and disruption of normal bone architecture, leading to increased mechanical fragility and fracture risk. The condition predominantly affects older individuals, especially postmenopausal women, in whom estrogen deficiency accelerates bone resorption.
Established risk factors include:
- Advanced age
- Female sex
- Low body mass index
- Sedentary lifestyle
- Smoking
- Inadequate nutritional intake
In women older than 60 years sustaining hip fractures, several modifiable contributors—such as reduced physical activity, smoking history, insufficient calcium intake, and absence of prior osteoporosis screening—have been documented (1), with very few patients having received prophylactic treatment before fracture occurrence. These observations underscore the necessity of proactive identification and early intervention in high-risk groups.
Importantly, osteoporosis should not be regarded solely as a reduction in bone density. It represents a disorder of bone quality involving architectural deterioration that significantly influences skeletal strength (2). Comprehensive fracture risk evaluation, therefore, requires assessment of both bone mass and microstructural integrity. Integrating these parameters into orthopaedic planning enhances risk stratification and informs more appropriate therapeutic strategies (2,3).
Rising Incidence and Gender Predilection
Osteoporosis is emerging as a major public health concern in India, disproportionately affecting women due to intersecting biological, nutritional, and sociocultural determinants. Estimates indicate that approximately 46 million Indian women over 50 years of age are affected, illustrating the scale of the problem (3). Despite this burden, diagnosis frequently occurs only after a fragility fracture, positioning orthopaedic surgeons as the first point of clinical contact.
Low-energy fractures of the hip, vertebrae, and distal radius are increasingly encountered among elderly women. Contributing factors include:
- Inadequate calcium intake
- Widespread vitamin D deficiency (4)
Limited sunlight exposure, dietary insufficiency, socioeconomic constraints, and hormonal changes during menopause collectively accelerate bone loss (4).
Cultural factors further compound the problem. Many women delay medical evaluation due to competing familial responsibilities, and routine screening remains uncommon even in high-risk groups (4). For orthopaedic surgeons, this translates into complex fracture configurations, diminished implant purchase, prolonged healing times, and increased complication rates.
Mitigating this disparity requires targeted strategies encompassing:
- Nutritional education
- Supplementation
- Systematic screening of postmenopausal women (4)
Although women represent the majority of cases, osteoporosis in men—often diagnosed later and presenting with severe fractures—must also be addressed. A comprehensive and gender-inclusive framework is therefore essential.
Pathological Insights Relevant to Orthopaedic Practice
Osteoporosis has profound implications for orthopaedic management because it directly influences fracture patterns, fixation stability, and postoperative outcomes. Beyond its metabolic basis, the disease modifies the mechanical behaviour of bone, thereby affecting surgical planning and long-term durability.
Pathophysiologically, osteoporosis involves both a reduction in BMD and qualitative microarchitectural deterioration, including trabecular thinning, fragmentation, and increased cortical porosity (5). These alterations predispose to fragility fractures involving the hip, spine, and distal forearm. Clinically, the condition often remains silent until a fracture occurs (6).
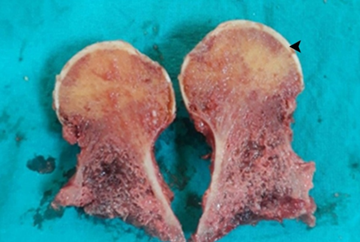
Figure A: Gross photograph of a longitudinally sectioned head of femur. The arrow highlights the cartilaginous cap.
Radiographs may underestimate bone fragility, as histologically compromised bone can appear only mildly osteopenic. Nevertheless, impaired microstructure reduces screw holding capacity, increases the risk of implant loosening, delays union, and predisposes to re-fracture, critical considerations during orthopaedic procedures.
Dual-energy X-ray absorptiometry (DEXA) remains the reference standard for BMD assessment (6). Incorporating opportunistic screening in fracture clinics and perioperative workflows enables early identification and secondary prevention (5).
Microscopic Alterations
At the tissue level, trabecular bone exhibits pronounced thinning and perforation, disrupting its lattice configuration and reducing load distribution capacity (7). Loss of trabecular number and connectivity increases intertrabecular spacing, with reported expansion from approximately 3–5 μm in healthy bone to 5–10 μm in osteoporotic specimens (8).
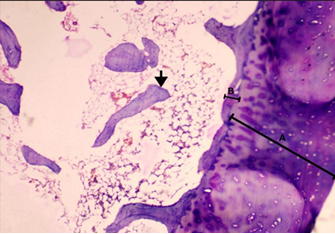
Figure B: Photomicrograph of the resected head of femur. Line A denotes the cartilaginous cap, which appears unremarkable. Line B indicates markedly thinned cortical bone. The arrow points to trabecular bone, showing reduced trabecular thickness with loss of inter-trabecular connectivity at multiple sites, consistent with osteoporotic changes.
Cortical bone undergoes parallel deterioration. Enhanced cortical porosity, particularly in regions such as the femoral neck and distal radius, significantly reduces bending strength (9). Alterations in the Haversian system impair remodelling efficiency (7). Prominent cement lines and evidence of increased endosteal resorption reflect accelerated turnover, while microfractures further disrupt trabecular continuity (9).
Although compensatory periosteal apposition may modestly increase bone diameter and partially offset strength loss, this adaptation rarely compensates for internal structural compromise (9).
Management requires coordinated multidisciplinary care. Pharmacological therapy includes:
- Anti-resorptive agents
- Anabolic medications
- Calcium and vitamin D supplementation
- Nutritional optimisation (10)
Orthopaedic surgeons are uniquely positioned to initiate evaluation during hospital admission for fracture management, transforming the peri-fracture period into an opportunity for secondary prevention. Surgical strategy must account for compromised bone quality through implant selection, augmentation techniques, and tailored rehabilitation protocols.
Biochemical Markers of Osteoporosis
In addition to imaging and histology, biochemical markers provide insight into the dynamic processes of bone remodelling. These indicators assist in assessing turnover status, estimating fracture risk, and monitoring therapeutic response.
- Procollagen type I N-terminal pro-peptide (PINP): Serves as a marker of bone formation, reflecting osteoblastic collagen synthesis. Elevated levels correlate with increased turnover and fracture susceptibility (11). PINP is particularly useful for evaluating response to anabolic and anti-resorptive therapies.
- Resorption markers: Such as C-terminal telopeptide (CTX) and N-terminal telopeptide (NTX) represent osteoclastic activity. Reduction in CTX levels following anti-resorptive therapy has been associated with decreased fracture incidence (12). Persistently elevated resorption markers may signal increased risk of delayed healing or implant-related complications.
Routine biochemical parameters also contribute valuable information:
- Serum calcium and phosphate concentrations influence bone mineralisation, and deficiencies may provoke secondary hyperparathyroidism (13).
- Vitamin D insufficiency, common in elderly populations, impairs bone strength and fracture healing (13).
- Bone-specific alkaline phosphatase reflects osteoblastic activity and may provide indirect insight into reparative capacity (11,13).
Although biological variability limits standalone diagnostic utility, combining biochemical markers with imaging and clinical assessment enhances comprehensive evaluation. Continued investigation is warranted to refine their integration into routine orthopaedic practice.
References
- Unay K, Demircay E, Akan K, Sener N. Risk factors for osteoporosis in women having hip fractures after 60 years of age. Acta Orthop Traumatol Turc. 2005;39(4):295–299. doi:10.3944/AOTT.V39I4.652
- Casciaro S, Renna MD, Pisani P, Greco A, Conversano F, Muratore M. New ultrasound-based methods for early osteoporosis diagnosis and fracture risk estimation. Int J Med Technol Innov Eng. 2014;4(2):24–38. doi:10.4018/IJMTIE.2014040103
- Khadilkar A, Mandlik R. Epidemiology and treatment of osteoporosis in women: an Indian perspective. Int J Womens Health. 2015;7:841–850. doi:10.2147/IJWH.S54623
- Sen S, Mookerjee M. Osteoporosis—are we aware? J Pharm Res. 2022;21(2):38–43. doi:10.18579/jopcr/v21i2.1
- Understanding osteoporosis: pathophysiology, risk factors, diagnosis, and management. Adv Aging Res. 2024;13(3):1–12. doi:10.4236/aar.2024.133003
- Theodorou SJ, Theodorou DJ, Sartoris DJ. Evaluation of osteoporosis in orthopaedic practice: a review of current diagnostic modalities. Am J Orthop. 2003;32(4):178–188.
- Kulikovsky, V. F., Pavlova, T. V., Bashuk, I. P., Pilkevich, N. B., & Pavlova, L. A. (2020). Morphofunctional Aspects of Bone Tissue at Osteoporosis. Systematic Reviews in Pharmacy, 11(6), 31–35. https://doi.org/10.31838/SRP.2020.6.07
- Kim, G.-J., Yoo, H. S., Lee, K. J., Choi, J.-W., & An, J. H. (2018). Image of the Micro-Computed Tomography and Atomic-Force Microscopy of Bone in Osteoporosis Animal Model. Journal of Nanoscience and Nanotechnology, 18(10), 6726–6731. https://doi.org/10.1166/JNN.2018.15472
- Török-Oance, R., Vasile, L., & Murgu, E. (2014). Aspects of bone tissue in osteoporosis. 17(2), 129–136.
- Reitman CA, Mathis KB, Heggeness MH. An orthopedic perspective of osteoporosis. In: Advances in Orthopaedics. Academic Press; 2008. p. 1555–1573. doi:10.1016/B978-012370544-0.50067-7
- Samavarchi Tehrani S, Moallem M, Ebrahimi R, Hosseini SR, Nooreddini H, Parsian H. Status of circulating bone turnover markers in elderly osteoporosis/osteopenia patients compared with healthy subjects. Asian Biomed. 2020;14(3):97–106. doi:10.1515/ABM-2020-0015
- Altınsoy KE, Unat B. The role of bone turnover markers in diagnosis, monitoring, and pathological fractures of osteoporosis. Ulus Travma Acil Cerrahi Derg. 2024;30(5):323–327. doi:10.14744/tjtes.2024.48409
- Yaribeygi H, Bayat N, Alishiri GH, Maleki M, Jamialahmadi T, Sahebkar A. Serum biochemical factors as indicators of osteoporosis: a cross-sectional study. 2024. doi:10.2174/0102506882303034240726061322
