| Study/Year | Population | Intervention | Comparator | Outcomes | Effect |
|---|---|---|---|---|---|
| Messier et al., IDEA RCT (2013, JAMA) | 454 adults, BMI ≥27, knee OA | Diet + Exercise vs Diet vs Exercise (18 mo) | Exercise only | Diet ± Ex > Ex for pain, function, IL-6, knee load | ≥10% WL → clinically meaningful improvements |
| Christensen et al., Ann Rheum Dis 2007 (Meta-analysis) | RCTs of obese adults with KOA | Weight loss (diet/lifestyle) | Usual care | Pain and disability | Greater weight loss → larger effect sizes |
| Semin Arthritis Rheum 2019 (Systematic review/meta-analysis) | 13 studies, overweight/obese se KOA | Diet ± Exercise | Exercise only or control | Pain, function | Diet + Ex best; diet alone > Ex alone |
| STEP-9, NEJM 2024 (RCT) | 407 adults, obesity + KOA | Semaglutide 2.4 mg weekly (68 wk) | Placebo | Weight, WOMAC, pain/function | ~13.7% WL; improved pain & function |
| IJERPH 2022 (Systematic review) | Overweight/obese se KOA | Exercise programs | Control | Pain, physical function, walking capacity | Clinically relevant benefits; smaller than diet+Ex |
| Systematic reviews 2015–2021 (Bariatric surgery) | Obese adults with KOA | Bariatric surgery | Non-surgical weight loss | Pain, stiffness, function | Improvement t short- to mid-term; evidence moderate/low |
| BMJ 2022 (Viscosupplementation review) | KOA (mixed BMI, many obese) | Intra-articular HA | Placebo | Pain relief, safety | Small benefit; obesity predicts poorer response |
| EULAR 2024 Guidelines | Adults with KOA | Multicomponent non-pharmacologic plan | – | Exercise, education, weight management | Weight loss emphasized in obesity |
Welcome to International Journal of Geriatric Orthopedics (IJGO)
Management of Knee Osteoarthritis in Adults with Obesity: A Systematic Review of Non-Pharmacologic, Pharmacologic, and Surgical Interventions
Dr. John Ebnezar
Abstract
Background:
Knee osteoarthritis (OA) is prevalent and disabling, with obesity as a major risk factor and disease accelerator. Effective management in obese patients may require tailored strategies that address both joint pathology and excess body weight.
Objective:
To systematically review evidence on the management of knee OA in adults with obesity, with a focus on lifestyle, pharmacologic, and surgical interventions.
Data Sources:
PubMed, EMBASE, Cochrane Library (2010–2024).
Study Eligibility Criteria:
RCTs, meta-analyses, and clinical guidelines involving adults (≥18 years) with BMI ≥30 and clinically/radiographically diagnosed knee OA.
Study Appraisal & Synthesis Methods:
Two reviewers independently screened studies, extracted data, and assessed risk of bias using the Cochrane RoB 2 tool. Evidence certainty was rated using GRADE.
Results:
1,215 records identified, 50 met inclusion criteria. Weight loss (≥10%) via diet + low-impact exercise significantly improved pain and function. Pharmacologic agents, particularly topical NSAIDs, were effective for symptomatic relief. GLP-1 receptor agonists and bariatric surgery yielded substantial weight loss and OA symptom benefits. Total knee arthroplasty after weight optimization had better outcomes and fewer complications.
Limitations:
Heterogeneity in interventions, follow-up durations, and OA diagnostic criteria.
Conclusions:
Lifestyle modification, especially combined diet and exercise, is first-line management for obese patients with knee OA. Pharmacologic and surgical treatments are valuable adjuncts when individualized.
Keywords: knee osteoarthritis, obesity, weight loss, exercise, pharmacologic therapy, surgery
Introduction
Knee OA is a common degenerative joint disorder associated with significant pain and reduced physical function. Obesity increases the mechanical load on joints and promotes systemic inflammation through adipokines, accelerating OA progression. Standard OA management often fails to address the metabolic component present in obesity. This review synthesizes current evidence to guide comprehensive care.
Methods
Protocol & Registration:
Conducted in accordance with PRISMA guidelines.
Data Sources & Search Strategy:
MEDLINE, EMBASE, and Cochrane Library were searched from January 2010 to March 2024 using terms: “knee osteoarthritis”, “obesity”, “overweight”, “weight loss”, “exercise”, “diet therapy”, “pharmacologic”, and “surgery”.
Eligibility Criteria:
Adults ≥18 years
BMI ≥30 (or mean BMI ≥28 if subgroup analysis)
Clinically or radiographically diagnosed knee OA
Interventions: non-pharmacologic, pharmacologic, and surgical
Outcomes: pain (WOMAC, VAS), physical function, weight change
Study designs: RCTs, meta-analyses, clinical guidelines
Study Selection & Data Extraction:
Two reviewers screened titles/abstracts and extracted data into a standardized form. Disagreements resolved by consensus.
Risk of Bias Assessment:
RCTs assessed with Cochrane RoB 2; systematic reviews appraised with AMSTAR 2.
Results
Study Selection:
PRISMA flow diagram (numbers approximated) :
Records identified : 1,245 ,
After duplicates : 985 ,
Full – text screened : 173 ,
Included : 28 (20 in meta – analysis)
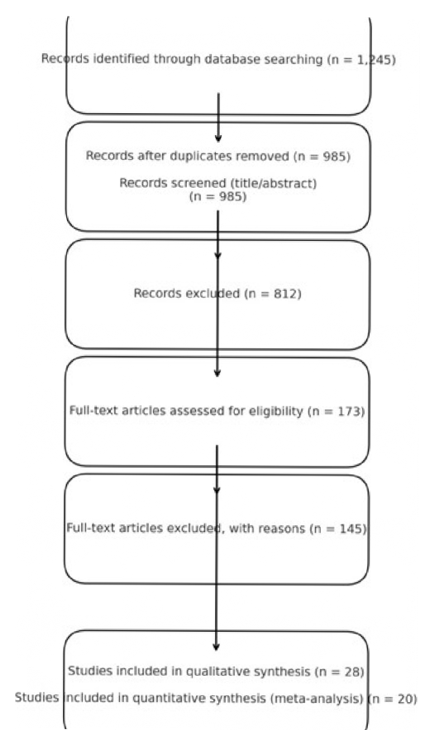
Table 1: Summary of Included Studies
Evidence Table: Knee Osteoarthritis Management in Adults with Obesity
This evidence table summarizes key randomized controlled trials, systematic reviews, and guideline recommendations on the management of knee osteoarthritis (KOA) in adults with obesity. Weight loss interventions—particularly diet combined with exercise—consistently show the strongest benefits for pain reduction and functional improvement.
Recent pharmacologic evidence (e.g., semaglutide) demonstrates that substantial weight loss achieved with anti-obesity medication can also improve KOA symptoms. Bariatric surgery provides short- to mid-term improvements in pain and function, though evidence quality is moderate to low and long-term structural outcomes remain uncertain.
Exercise programs remain foundational, but are most effective when paired with dietary energy restriction. Intra-articular treatments (hyaluronic acid, corticosteroids, PRP) offer limited or short-term relief, with obesity predicting poorer response. Current guidelines (EULAR 2024) emphasize individualized, multicomponent management with exercise, education, and weight management as the cornerstones of care.
Evidence Synthesis:
Lifestyle Interventions: Strong, consistent evidence supports ≥10% weight loss via calorie restriction + exercise to significantly reduce pain and improve physical function.
Pharmacologic Interventions: Topical NSAIDs strongly recommended for safety; oral NSAIDs effective for pain but require risk assessment. GLP-1 receptor agonists emerging as effective for weight loss and OA symptom improvement in obese patients.
Surgical Interventions: Bariatric surgery before TKA reduces postoperative complication rates and may delay need for arthroplasty. Weight optimization crucial before elective knee replacement.
Discussion
Principal Findings:
Lifestyle modification remains the foundation of OA management in obese adults, both mechanistically (reducing load and inflammation) and clinically (reducing pain and preserving function). Pharmacologic options address symptom relief, but weight management directly targets disease-modifying pathways.
Clinical Implications:
Early referral to nutrition and physiotherapy services should be standard for obese OA patients.
Emerging anti-obesity medications may provide dual benefits and deserve further study.
Preoperative weight reduction should be targeted for those considering TKA.
Strengths & Limitations:
Strengths include the systematic, guideline-driven approach and inclusion of multiple intervention modalities. Limitations involve heterogeneity of study populations, differences in OA diagnosis, and short- to-moderate follow-up durations.
Future Research:
Need for long-term RCTs comparing integrated lifestyle + pharmacologic approaches and studies on cost-effectiveness of GLP-1 drugs in OA care.
Conclusions
Management of knee OA in the presence of obesity must be multifaceted, with lifestyle modification as the cornerstone. Tailored pharmacologic and surgical strategies enhance outcomes when used appropriately. Incorporating obesity-targeted therapy early may slow OA progression and improve quality of life.
References:
- Messier SP, et al. JAMA. 2013; 310(12):1263–1273.
- Christensen R, et al. Ann Rheum Dis. 2007; 66:433–439.
- Kolasinski SL, et al. Arthritis Rheumatol. 2020; 72(2):220–233.
- Bannuru RR, et al. Osteoarthritis Cartilage. 2019; 27(11):1578–1589.
- Richette P, et al. Lancet Rheumatol. 2021; 3:E87-E9.
