| Parameter | Number |
|---|---|
| Number of patients with knee pain | 96 |
| Number of male patients | 42 |
| Number of female patients | 54 |
| Number of patients managed conservatively | 68 |
| Number of patients managed operatively | 28 |
Welcome to International Journal of Geriatric Orthopedics (IJGO)
Exploring the Impact of Osteoporosis in Causing Osteoarthritis Knee: Genu Anoikodomisi as a Surgical Technique in the Management
Dr. Prabodh Kumar Dake, Dr. Chalumuri Navya, Dr. Bhaswanth Dake, Dr. S. Lavanya Kumari, Dr. Surya Prakash Naidu Paila
Abstract
Knee osteoarthritis (OA) is a prevalent form of arthritis that affects approximately 10% of individuals over 60 years of age worldwide. This condition significantly diminishes the quality of life of affected individuals, leading to symptoms such as joint pain, stiffness, crepitus, swelling, and limited mobility. Unfortunately, there is a common misconception among many physicians that osteoarthritis is solely a result of joint degeneration due to ageing. This misconception overlooks the multifaceted nature of the disease. Knee osteoarthritis often arises from the failure of periarticular tissues in the knee joint, especially the subchondral bone collapse due to osteoporosis, and the sarcopenia of periarticular muscles associated with old age.
Introduction
Knee osteoarthritis is not simply a disorder of a single tissue, such as articular cartilage, rather, it is a mechanical failure of the entire knee joint, involving one or more tissues within the joint. When any of the joint-supporting structures fail, wear and tear begin, leading to increased intra-articular stress that can damage the articular cartilage.
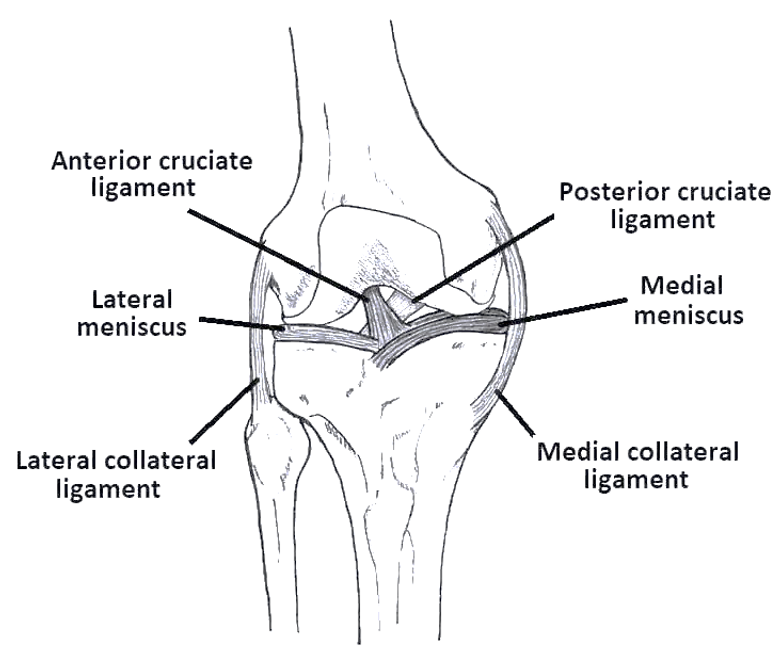
Why the Knee Joint is Predisposed to Osteoarthritis
The knee joint is constituted with three bones, three compartments and it is a triaxial joint. The knee is a remarkable weight-bearing and load-bearing joint, consisting of the articulation between the distal femur, proximal tibia, and patella. Its unique structure is supported by the surrounding muscles, which handle ground reaction forces from below and body reaction forces from above. The knee plays a pivotal role in providing support to the body in both dynamic and static scenarios. Unlike the hip and ankle joints, which are more stable and secure, the knee is relatively less secured and must balance the forces from above and below. As a result, the knee is subjected to greater stress during everyday physical activities compared to the hip and ankle joints.
Knee as the Centre of Force
Both ground reaction forces and body reaction forces traverse the knee during ambulation and stance. This places the knee at the centre of all forces and stresses. The hip and ankle joints significantly impact the health and function of the knee. The forces experienced by the knee vary depending on the activity; for instance, they can be half the body weight during normal walking and increase to over three times the body weight during stair climbing. Squatting places a significant patellofemoral joint reaction force on the knee.
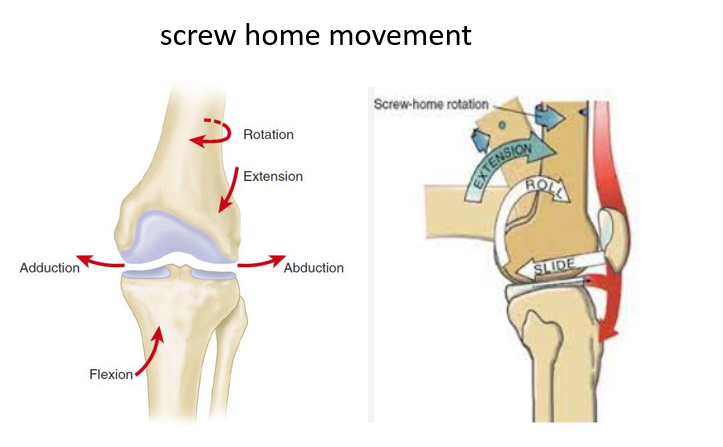
Functional Range of Motion (ROM) at the Knee
The knee’s motion is not a simple hinge-like flexion and extension. Instead, it involves three separate planes of motion during the gait cycle, referred to as “triaxial motion.” In addition to sagittal plane flexion and extension, the knee experiences abduction and adduction in the coronal plane and internal and external rotation in the transverse plane.
Risk Factors
Several risk factors contribute to the development of knee osteoarthritis, including excessive use of the knees, obesity, sarcopenia, osteoporosis, and preexisting mechanical axis alterations. These risk factors can lead to abnormal joint stress and mechanical changes within the knee joint.
Knee as a Load-Bearing Joint
The knee is primarily a load-bearing joint, not just a weightbearing joint. While the body mass plays a role, the majority of the load on the knee joint results from the strength of periarticular muscles and adjacent bones. The concentration of force and the rate of loading are critical factors in the development of osteoarthritis. As age advances, the quality of periarticular bone decreases due to osteoporosis, and the tone of periarticular muscles diminishes due to sarcopenia, both of which can lead to abnormal joint stress and knee joint damage.
Mechanical Environment’s Influence on Knee Health
The mechanical environment experienced by the knee during walking influences the health of all knee-supporting structures, including articular cartilage. Healthy cartilage is conditioned to loading and repetitive cycles of loading during walking, maintaining cartilage homeostasis as long as there are no deviations from normal patterns of locomotion, knee joint structure, or cartilage biology.
Articular Cartilage
Articular cartilage is unique as it is avascular, alymphatic, and aneural tissue. It is resilient and can withstand various forms of stress. The balance between the synthesis and degradation of proteoglycans and collagens is essential for cartilage maintenance. The cartilage’s proteoglycans retain water and the collagen resists tensile forces within the matrix. The structure of the cartilage is crucial for load-bearing.
Osteochondral Unit
The functional unit of a synovial joint, known as the “osteochondral unit,” comprises hyaline cartilage and subchondral bone. The health of this unit is largely dependent on the subchondral cancellous bone’s condition and the surrounding periarticular structures. Subchondral bone serves as a primary source of nutrition for cartilage. Subchondral bone absorbs loads and plays a key role in supporting cartilage while absorbing shock. Damage to the subchondral bone, such as microfractures from osteoporosis, can lead to the thinning and sclerosis of subchondral bone, increasing the load on the articular cartilage.
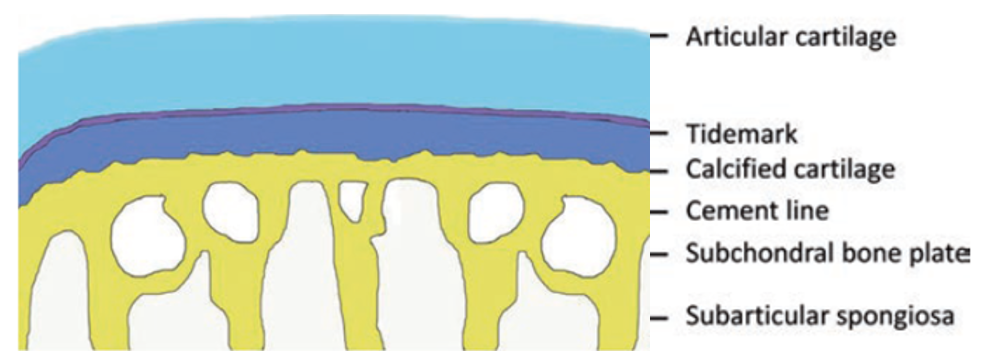
Osteochondral Unit — Functional Unit of Joint
Dysfunction in one component may affect all the components.
The Strength of the Bone and the Joint
The strength of the knee joint is closely linked to the bone’s mineral density, which provides support for muscles, ligaments, menisci, and cartilage. Changes in subchondral bone due to osteoporosis can significantly impact the mechanical axis of the knee. Osteoporosis can lead to microfractures in the subchondral cancellous bone, resulting in collapse and sclerosis, which subsequently increases the load on the medial compartment of the knee and thins the articular cartilage. Therefore, thinning of the articular cartilage can be attributed to changes in the subchondral cancellous bone caused by osteoporosis. The strength of the bone is the strength of the joint ………Role of osteoporosis
The strength of the bone is the strength of the joint ……… Role of osteoporosis
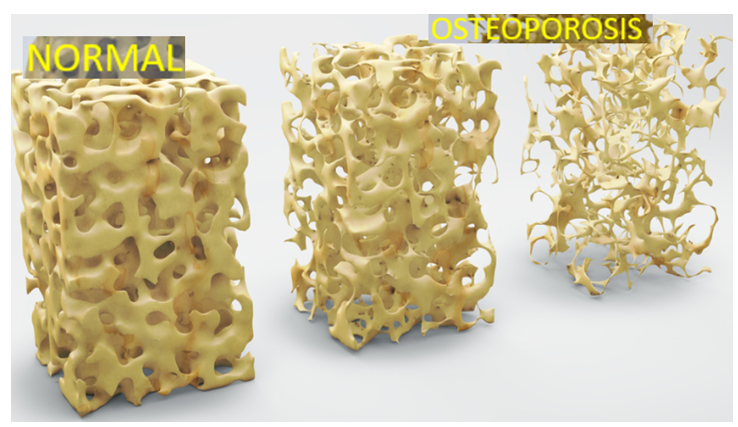
Osteoporosis and Sarcopenia
The normal knee joint can support a life time of repetitive load without the development of mechanical changes. The strength of the bone and muscle is the strength of the joint. sarcopenia or osteoporosis, may increase shear stress at the bone and cartilage interface precipitating cartilage degradation. Load bearing capacity of joint depends on strength of the bone and strength of the muscle. Osteoporosis and Sarcopenia cause early muscle fatigue and failure of load bearing capacity thus load falls directly on joints (knee) Osteoporosis and sarcopenia reduce the knee joint’s weightbearing and load-bearing capacity, leading to inadequate shock absorption and increased intra-articular stress, contributing to knee joint mechanical failure. Osteoporosis directly weakens bone strength and indirectly influences joint strength.
Articular Cartilage, Viscoelasticity, and Repetitive Impulsive Loading
Articular cartilage depends on a delicate balance of load and interstitial fluid flow for its function. Healthy cartilage can transmit load to the underlying subchondral bone without causing damage. Repetitive impulsive loading (RIL) can be detrimental to cartilage as it does not allow sufficient time for interstitial fluid to flow and absorb transmitted energy. The normal subchondral bone is viscoelastic. In addition to the viscoelasticity of sub chondral bone, timely contraction of periarticular muscles plays a crucial role in protecting the joints against RIL.
Softening of Subchondral Bone and Cartilage Damage:
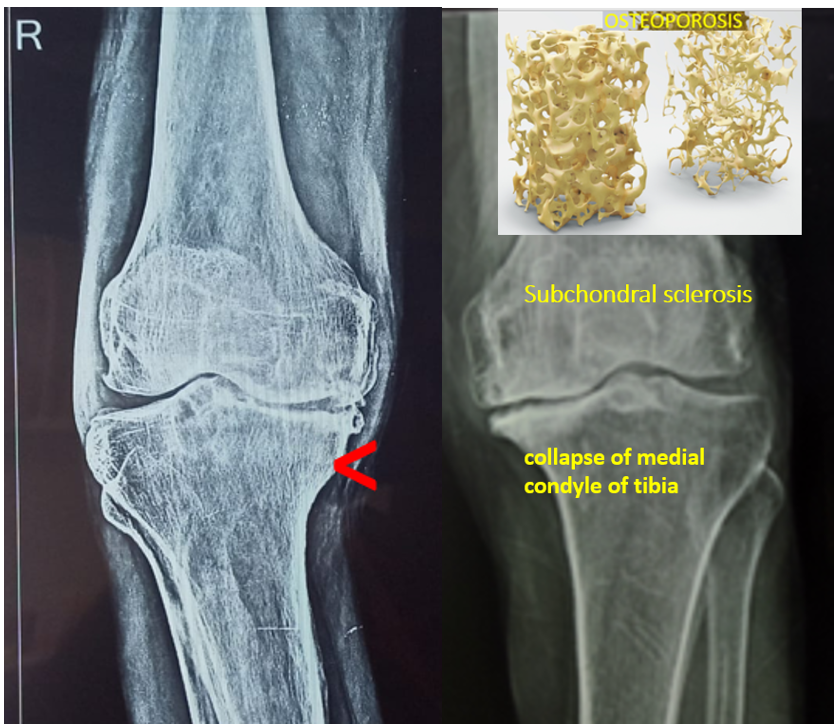
Subchondral bone plays a key role in supporting the articular cartilage mechanically and metabolically and absorbing shock. Subchondral bone attenuates about 30% of loads through joints while articular cartilage attenuates only 1.3% of them. Subchondral bone undergoes remarkable changes in both composition and structural organization due to osteoporosis. Porotic sub chondral cancellous trabeculae starts collapsing by micro fractures on weight bearing. The softening of the underlying subchondral bone and the healing of trabecular microfractures can lead to subchondral sclerosis. Sclerotic subchondral bone is not viscoelastic and overlying cartilage loses its nutrition and cartilage break down may start. . The sub chondral sclerosis happens before the articular cartilage starts to wear away. Therefore, cartilage damage can be preceded by subchondral bone collapse and sclerosis.
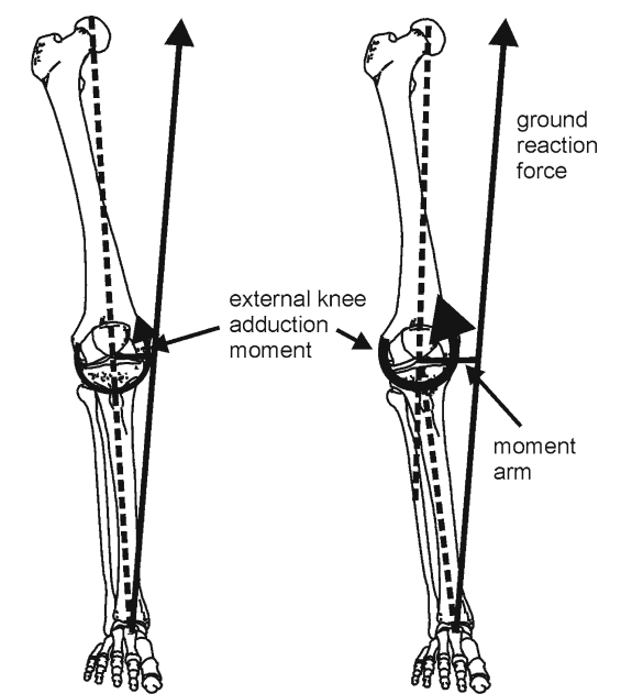
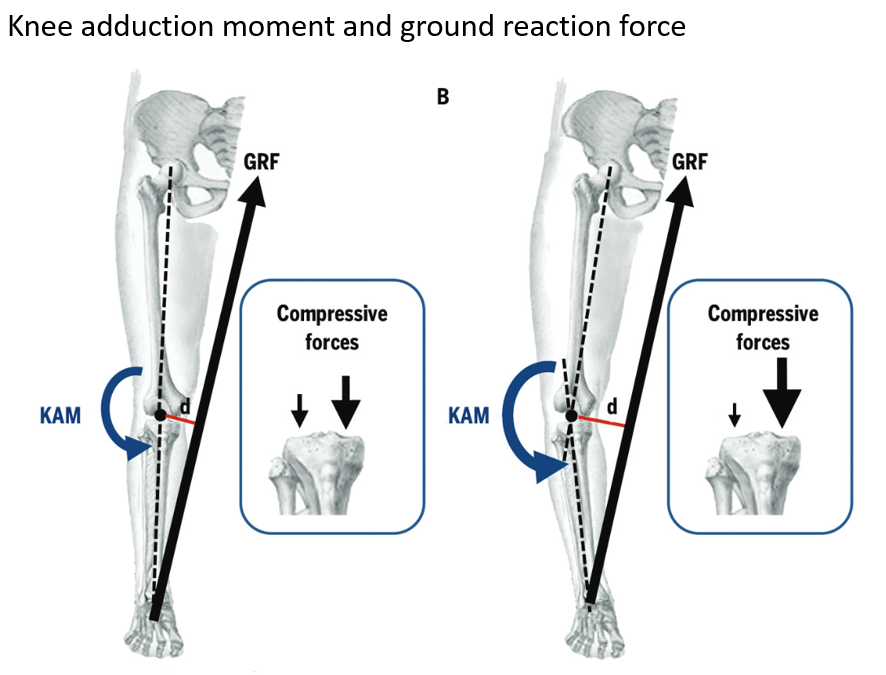
Medial Condyle of Tibia and Mechanical Axis Deviation:
Osteoporosis is the principal cause for the collapse of sub chondral trabeculae especially in medial condyle of tibia can lead to the alteration of the convex shape to a straight or concave shape. Viscoelasticity of the subchondral bone is lost. Which lead to deviation of mechanical axis. This deviation can lead to a higher adduction moment, raise in intra articular stress and more load on medial compartment. Normal mechanical axis is essential for equal weight distribution in the medial and lateral tibiofemoral compartments during the stance phase, but it deviates from the midline due to bony changes resulting from the collapse of thinned cancellous trabeculae more in medial tibial condyle which receives the load. Medial tibial condyle has no support like lateral tibial condyle by head of the fibula through superior tibiofibular joint. Hence medial tibial condyle is subjected for more stress.
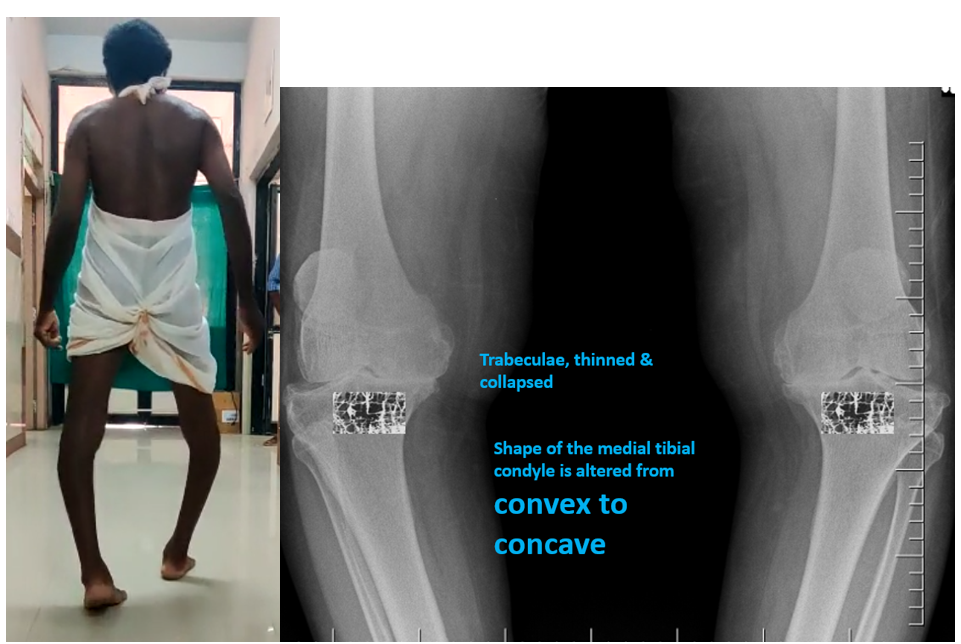
CONVEXITY OF MEDIAL CONDYLE OF TIBIA IS ALTERED DUE TO COLLAPSE OF THINNED CANCELLOUS TRABECULAE
Medial tibial condyle …… Convexity >>>>>>> Straight >>>>>>> Concavity
Right knee gross varus with lateral thrust while walking, varus angle is at medial condyle of Tibia Most of the times, varus at knee in older people is not due to medial joint compartment narrowing. But it is due to collapse of sub chondral cancellous bone due to osteoporosis more on medial condyle of tibia which receives the load and weight
CAUSE OF PAIN at KNEE in OA
Micro fractures of porotic sub chondral cancellous trabeculae causes pain and pain at knee may be mistaken for OA knee pain. Subchondral sclerosis results in intramedullary venous hypertension – a major cause of pain at knee. Sometimes pain may arise from stretching of nerve endings in the periosteum covering osteophytes. As the articular cartilage is AVSCULAR, ANEURAL and ALYMPHATIC, its breakdown can’t produce pain.
- Clearly showing ….. sub chondral trabeculae collapse at medial condyle of tibia results in varus

So thinned cancellous trabeculae break and collapse cause pain - Prolonged walking …… knee pain
- Prolonged squatting …….. Knee pain
- Climbing stairs ……. Knee pain
- Getting up from sitting posture ……. Knee pain
- Prolonged standing … knee pain
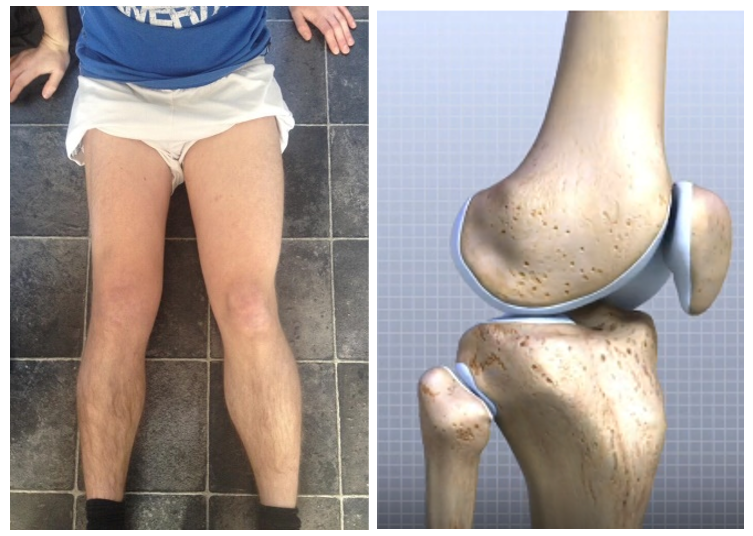
Quadriceps Wasting:
Quadriceps wasting is a common occurrence in individuals with knee osteoarthritis, which further diminishes the ability to support and stabilize the joint. In our study most of the patients are presenting with quadriceps wasting which reduces load-bearing capacity of the knee and further affects the stability of the joint. Then the load and weight directly fall on condyles of tibia, more on medial condyle of tibia as it has no support like lateral condyle by fibula through superior tibiofibular joint.
How to Recognize Osteoporosis Clinically:
Osteoporosis is a significant cause of knee pain that can lead to osteoarthritis. Clinical signs of osteoporosis-related to knee pain include pain and tenderness at proximal and distal parts of tibia especially over medial aspect as it is subcutaneous. Tenderness at distal radius on ventral aspect, and reduction in grip strength are also other features of osteoporosis. Back pain, neck pain, bilateral shoulder pains are also observed in geriatric people may be due to osteoporosis and sarcopenia. Collapse of sub chondral bone by micro fractures of thinned out trabeculae due to osteoporosis, gives pain and patient complains of pain knee which may be mistaken for OA knee pain.
PATIENTS AND METHODS
Study conducted in three years period (2020-2022) Evaluation of pain at knee in 96 patients both male and female of 50 years to 70 years age group.
Investigations
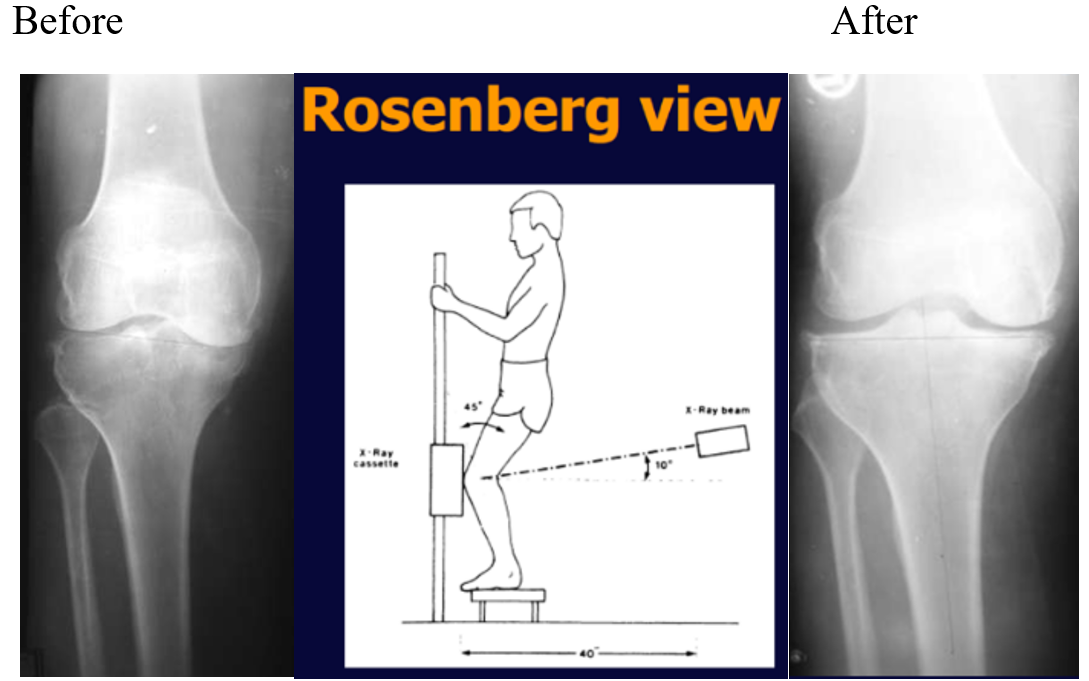
Basic investigation is Xray knee ……. AP and Lateral and Rosenberg views increased density of the subchondral bone (sclerosis) may occasionally be the first radiographic finding in osteoarthritis. Subchondral sclerosis is a thickening and hardening of bone that happens underneath cartilage in a joint before articular cartilage wear. Altered shape of the medial tibial condyle from convex to concave and reduced height of medial tibial condyle due to collapse of thin subchondral cancellous bone by micro fractures due to osteoporosis is another common observation.
Regular AP view of knee may show narrowing of medial joint space and it is due to tilt of tibial plateau which is resulted from collapse of subchondral bone due to osteoporosis. To know exact joint space Rosenberg view of the knee is mandatory.
To address knee osteoarthritis and its underlying causes, the following treatment goals are recommended:
Treatment Goals:
- Unloading of knee joint by life style modification and knee braces
- Improve bone strength by osteoporosis treatment, by injection Teriparatide, Vit D3, calcium supplements, protein-rich diets and physical activity
- Increase muscle strength by physiotherapy and exercises.
Surgery —- Anoikodomisi ……
Correction of mechanical axis deviation by open wedge osteotomy.
Address subchondral sclerosis by curetting and filling the subchondral space with cancellous bone graft.
Support open wedge osteotomy with tricortical bone graft from the iliac crest to prevent collapse of open wedge.
Conservative management …. radiological observations


Genu Anoikodomisi as a surgical note in the management of Osteoarthritis
(Genu in Latin means knee, Anoikodomisi in Greek means reconstruction) Reconstructing the collapsed medial condyle of the tibia involves performing an open wedge osteotomy. This procedure includes removal of the sclerosed subchondral bone by curettage and replacing it with a cancellous bone graft. Then supporting the open osteotomy by a tricortical bone graft from iliac crest to prevent further collapse. Additionally, fibrosed periarticular tissues can be released, and osteophytes can be excised.
Pre operative Right Knee OA

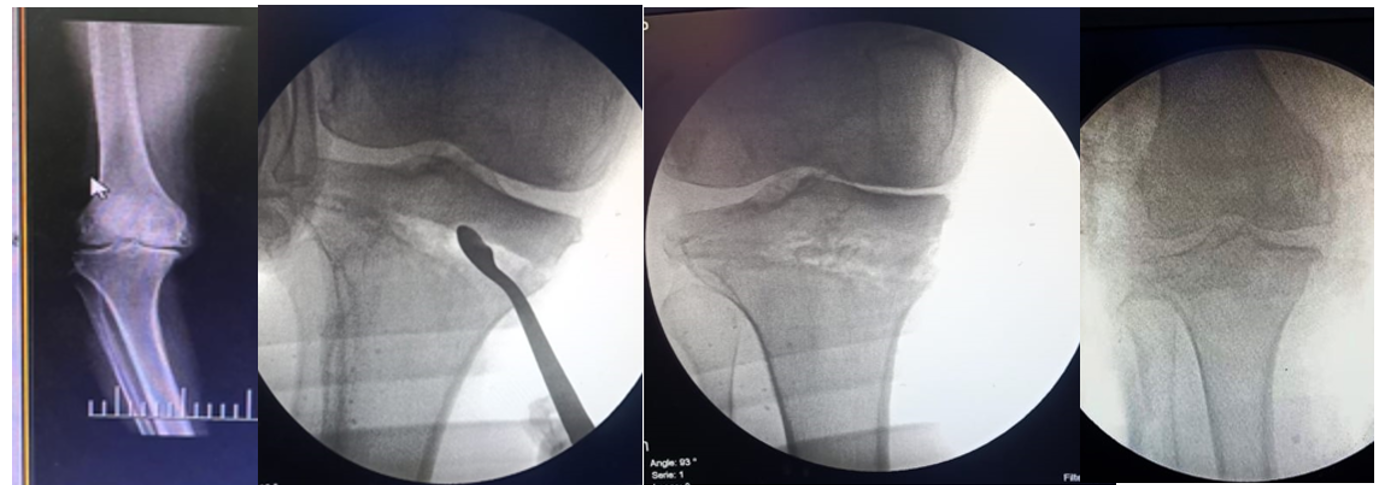
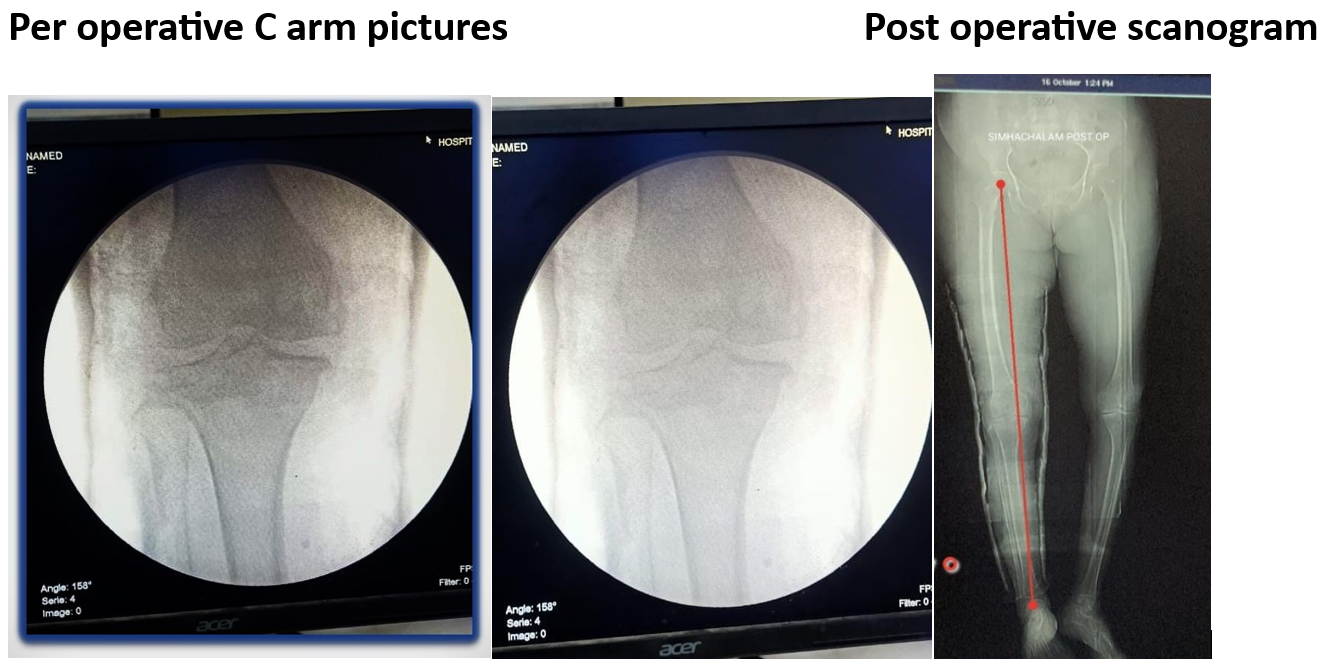
Open wedge osteotomy done, sub chondral sclerosis curetted, open wedge osteotomy supported with tricortical bone graft from iliac crest after sub chondral space filled with cancellous bone

After the surgery, immobilize the knee for a duration of eight weeks. During this period, we recommend engaging in static exercises to enhance the strength of the limb muscles. Additionally, we suggest the administration of Teriparatide injections and calcium supplements to fortify the bones. Following the eight-week immobilization, non-weight-bearing exercises are recommended for the subsequent two weeks. Then the initiation of weight-bearing activities will be contingent upon a satisfactory check x-ray, which typically occurs at the ten-week mark.

Once the weight-bearing axis is appropriately corrected and the knee is relieved of load (unloading of knee joint) for a period of two months, the thinned-out articular cartilage is expected to return to its normal state. The reduction of intraarticular mechanical stress plays a crucial role in promoting the repair process and healing of the osteochondral unit, providing relief from joint pain and enhancing overall joint function.
Out of 96 patients, 26 patients were selected for surgery. Criteria for surgery are pain at knee with mechanical axis deviation, limitation of knee flexion, limitation of patella mobility, reduced physical activity, difficulty in walking. If the patient is having severe articular cartilage damage confirmed by cartigram, TKR is the best option.
Results
All patients treated by both conservative and operative methods are doing well. No pain, no limp. Two patients are left with limitation of flexion about 20 degrees. Life style modification, regular exercises, rich protein diet should be continued. Patients should have awareness about osteoporosis and better to have regular checkups for any discomfort. All 96 patients received injection teriparatide for a period of six months to twelve months.
- My study reveals …….. Most of the times, varus at knee in older people is not due to medial joint space narrowing
- But it is due to collapse of sub chondral cancellous bone due to osteoporosis more on medial condyle of tibia which receives the load.
- Which further increases the load on medial compartment of knee leads to sub chondral sclerosis which in turn causes more pressure on articular cartilage and makes it thin. At this stage medial joint space appears narrow and knee joint looks varus.
- Collapse of sub chondral bone by micro fractures of thinned out trabeculae due to osteoporosis, gives pain and patient complains of pain knee which may be mistaken for OA knee pain
- Collapse of sub chondral bone by micro fractures of thinned out trabeculae due to osteoporosis, gives pain and patient complains of pain knee which may be
Discussion
Osteoporosis has definite impact in causing osteoarthritis of knee. On weight bearing thin subchondral cancellous bone may collapse due to micro fractures which in turn leads to subchondral sclerosis. This may interfere with the nutrition of articular cartilage. Hence cartilage damage was preceded by subchondral bone collapse.
By significantly limiting the loading of the unstable limb through prompt immobilization and unloading of the knee joint, the progression of osteoarthritis can be effectively prevented. Immobilization serves as an effective measure to reduce instability and intraarticular stress, offering a protective mechanism against the development of osteoarthritis.
The preservation of knee joints from osteoarthritis involves the prevention of its progression through measures such as strengthening of antigravity muscles and improving bone quality by giving teriparatide injections for six months to twelve months. This study underscores the importance of increasing awareness, advocating for improved screening of osteoarthritis, initiating early treatment, and actively working to prevent the progression of knee osteoarthritis.
Conclusion
Osteoarthritis of knee is not a disease of single tissue like articular cartilage but it is a mechanical failure of knee joint as a whole especially due to weakness of muscles and bones (sarcopenia and osteoporosis). As the articular cartilage is avascular, aneural and alymphatic it depends on subchondral bone for its nutrition. As long as sub chondral bone is healthy, articular cartilage will be good.
Subchondral bone plays a key role in mechanically and metabolically supporting the articular cartilage and absorbing shock. Subchondral bone is incredibly important for the functioning of articular cartilage. Subchondral bone attenuates about 30% of loads through joints while cartilage attenuates only 1.3% of them. Subchondral trabecular bone has bone marrow houses mesenchymal stem cells (MSCs) with chondrogenic potential.
Hence osteochondral unit should be a focus of treatment and consider the subchondral bone condition in the treatment of osteoarthritis, with the aim of restoring the function of osteochondral unit for the joint preservation. In our study sub chondral part of the osteochondral unit is playing a major role for the strength of articular cartilage which is very much affected by osteoporosis. Excessive loading of a joint will lead to subchondral bone collapse before it produces obvious damage to articular cartilage. Hence cartilage damage was preceded by sub chondral bone collapse.
Our basis research is the prevention of progression of osteoarthritis by reducing the increased intraarticular stress that is causing joint damage as a whole and preservation of joint rather than treating damage of articular cartilage.
References:
- Shelburne KB, Torry MR, Pandy MG. (2006) Contributions of muscles, ligaments, and the ground-reaction force to tibiofemoral joint loading during normal gait.
- Andriacchi, Thomas P. et al. (2009) Gait Mechanics Influence Healthy Cartilage Morphology and Osteoarthritis of the Knee.
- Harada Y, Weavers HW, Cooke TD. Distribution of bone strength in the proximal tibia.
- Madry H, Orth P, Cucchiarini M. (2016) Role of the subchondral bone in articular cartilage degeneration and repair.
- Kawcak CE, McIlwraith CW, Norrdin RW, Park RD, James SP. The role of subchondral bone in joint disease: a review. Equine Vet J. 2001;33:120–6.
- Goldring SR, Goldring MB. Changes in the osteochondral unit during osteoarthritis: structure, function and cartilage-bone crosstalk. Nat Rev Rheumatol. 2016;12:632-44.
- Madry H, Orth P, Cucchiarini M. Role of the subchondral bone in articular cartilage degeneration and repair. J Am Acad Orthop Surg. 2016;24:e45-6.
- Orth P, Cucchiarini M, Kohn D, Madry H. Alterations of the subchondral bone in osteochondral repair-translational data and clinical evidence. Eur Cell Mater. 2013;25:299-316. discussion 314-296.
- Imhof H, Breitenseher M, Kainberger F, Rand T, Trattnig S. Importance of subchondral bone to articular cartilage in health and disease. Top Magn Reson Imaging. 1999;10:180-92.
- Li G, Yin J, Gao J, Cheng TS, Pavlos NJ, Zhang C, Zheng MH. Subchondral bone in osteoarthritis: insight into risk factors and microstructural changes. Arthritis Res Ther. 2013;15:223.
- Cerejo R, Dunlop DD, Cahue S, Channin D, Song J, Sharma L. The influence of align-ment on risk of knee osteoarthritis progression according to baseline stage of disease. Arthritis Rheum. 2002;46(10):2632–6.
- Moyad TF, Minas T. Opening wedge high tibial osteotomy and Fujisawa Y, Masuhara K, Shiomi S. The effect of high tibial osteotomy on osteoarthritis of the knee. An arthroscopic study of 54 knee joints. Orthop Clin North Am. 1979;10(3):585–08.
- Mina C, Garrett WE Jr, Pietrobon R, Glisson R, Higgins L. High tibial osteotomy for un-loading osteochondral defects in the medial compartment of the knee. Am J Sports Med. 2008;36(5):949–55.
- Rodner CM, Adams DJ, Diaz-Doran V, et al. Medial opening wedge tibial osteotomy and the sagittal plane: the effect of increasing tibial slope on tibiofemoral contact pressure. Parker DA, Beatty KT, Giuffre B, Scholes CJ, Coolican MR. Articular cartilage changes in patients with osteoarthritis after osteotomy.
